
Dual antiplatelet therapy (DAPT) is a mainstay for myocardial infarction (MI) therapy. However, in patients with myocardial infarction with non-obstructive coronary artery disease (MINOCA), clear recommendations are lacking in the literature. This study aims to identify the cases in which DAPT is currently prescribed at discharge for MINOCA.
MethodsThe authors analyzed a cohort of patients from a multicenter national registry enrolling patients who suffered their first MI between 2010 and 2017, and underwent coronary angiography revealing absence of stenosis ≥50%. Individual antithrombotic therapy was identified. A logistic regression analysis was applied to search for predictors of DAPT.
ResultsFrom a total of 16 237 patients analyzed, 709 (4.4%) were categorized as MINOCA. Mean age was 64±13 years, 46.3% (n=409) were females. 390 (55.0%) of MINOCA patients were discharged on DAPT. Males (OR 1.67, CI 95 [1.05-2.38], p=0.027), active smokers (OR=1.82, CI 95 [1.05-3.16], p=0.033), previous percutaneous intervention (OR 3.18, CI 95 [1.48-6.81], p=0.003), ST elevation MI (OR 2.70, CI 95 [1.59-4.76], p<0.001) and sinus rhythm at admission (OR=3.94, CI 95 [2.07-7.48], p<0.001) were independent predictors of DAPT use.
ConclusionIn this nationwide registry, DAPT was prescribed at discharge in 55% of MINOCA patients. Beyond sinus rhythm, the variables presented as independent predictors for DAPT use identify subgroups of patients who are classified as more prone to thrombotic events. The issue of how to handle antithrombotic agents in MINOCA patients is a topic open for discussion.
A dupla antiagregação plaquetar (DAPT) assume um papel central no tratamento dos doentes com enfarte agudo do miocárdio (EAM). Não há, no entanto, indicações claras para o tratamento de doentes com EAM sem doença coronária obstrutiva (MINOCA). Este artigo tem por objetivo identificar em que doentes com MINOCA é atualmente prescrita DAPT.
MétodosOs autores analisaram uma coorte de doentes de um registo nacional multicêntrico incluindo doentes com um primeiro EAM entre 2010 e 2017 e que realizaram coronariografia que revelasse ausência de qualquer estenose ≥50%. A terapêutica antitrombótica individualizada foi identificada e, de forma a determinar preditores da utilização de DAPT, uma regressão logística foi aplicada.
ResultadosDe 16 237 doentes, 709 (4,4%) foram classificados como MINOCA. A idade média foi 64±13 anos, 46,3% do género feminino. Dos doentes com MINOCA 390 (55,0%) tiveram alta hospitalar sob DAPT. O género masculino (OR 1,67, 95CI [1,05-2,38], p=0,027), ser fumador ativo (OR=1,82, 95CI [1,05-3,16], p=0,033), ter pelo menos uma intervenção coronária percutânea prévia (OR 3,18, 95CI [1,48-6,81], p=0,003), o diagnóstico de EAM com supradesnivelamento do segmento ST (OR 2,70, 95CI [1,59-4,76], p<0,001) e a presença de ritmo sinusal à admissão (OR=3,94, 95CI [2,07-7,48], p<0,001) foram os preditores independentes para a utilização de DAPT.
ConclusãoNeste estudo baseado num registo nacional, DAPT foi prescrita à alta a 55% dos doentes com MINOCA. Para além da presença de ritmo sinusal, os preditores independentes de utilização de DAPT identificam um subgrupo de doentes habitualmente classificado como tendo maior risco de eventos trombóticos. A questão de como lidar com o esquema antitrombótico de doentes com MINOCA permanece um tópico em discussão.
Dual antiplatelet therapy (DAPT) is one of the mainstays of medical management in patients with acute coronary syndrome (ACS).1,2 However, when a myocardial infarction (MI) occurs in the absence of obstructive coronary artery disease (CAD), the role of DAPT is not established. In 2017, the first authoritative international expert opinion was published by the European Society of Cardiology (ESC), defining myocardial infarction with non-obstructed coronary artery (MINOCA) as a working diagnosis – an MI in the absence of obstructive CAD on angiography in any potential infarct-related artery (no coronary artery stenosis ≥50%), and no clinically overt specific cause for the acute presentation.3 Our group has already published the first trial studying Portuguese MINOCA patients, identifying a mortality rate of nearly 9% in a three-year follow-up of our single- experience.4 Recently, the ESC included a chapter dedicated to MINOCA patients in the 2017 guidelines for the management of acute MI in patients presenting with ST-segment elevation1 as well as in the fourth universal definition of MI.5 It is highlighted that this is a working diagnosis requiring specific investigation and treatment. However, there are still no clear treatment guidelines, and the ESC states that more research into this topic is required. The only trial to date addressing this issue reported a neutral benefit for DAPT,6 and the first randomized controlled trial is currently in development (the MINOCA-BAT trial, ClinicalTrials.gov identifier NCT03686696). Thus, the present study aims to answer the following question: In which MINOCA patients do clinicians currently believe that DAPT can be useful?
MethodsThe Portuguese Registry of Acute Coronary Syndromes (ProACS) is an observational nationwide multicenter registry enrolling adult patients (>18 years) with an episode of ACS (ClinicalTrials.gov identifier NCT01642329).7,8 According to the current universal definition of MI, only type 1 MI patients are eligible.5 Demographic data, medical history, presenting symptoms, biochemical, electro and echocardiography data, pharmacological therapies, invasive procedures, in-hospital complications and mortality are collected using a standardized data collection form. The National Ethics Committee for Clinical Research, the institutional ethics committee and review board of each center approved individual participation in the registry.
The authors analyzed the ProACS database for patients with a first MI enrolled between 2010 and 2017, including only patients who underwent a coronary angiography revealing absence of any lesion causing ≥50% luminal reduction. The primary endpoint was DAPT prescription at discharge. Valvular heart disease was defined according to current guidelines,9 and included in the analysis if it presented at least moderate severity. The definitions of registry variables have already been published in the literature.7,8 Regarding statistical analysis, categorical variables are presented as frequency values and continuous variables are presented as mean (μ) ± standard deviation. Due to sample size, normal distribution of variables was assumed and parametric tests were used for between-group comparison. Comparisons between groups were made for each included variable with a known result, by using a chi-square test or a Student's t-test when appropriate. Statistical significance was defined as a p-value <0.05. To better represent the antiplatelet strategy of the attending cardiologists, data regarding the use of DAPT in-hospital and at discharge were also compared. In order to determine the independent predictors for DAPT use at discharge, a multivariate logistic regression analysis with stepwise-forward method was performed for each group, including all pharmacological treatment and also pre-hospital, clinical and laboratorial data, ACS classification and coronary anatomy. Model calibration was assessed with the Hosmer-Lemeshow test.
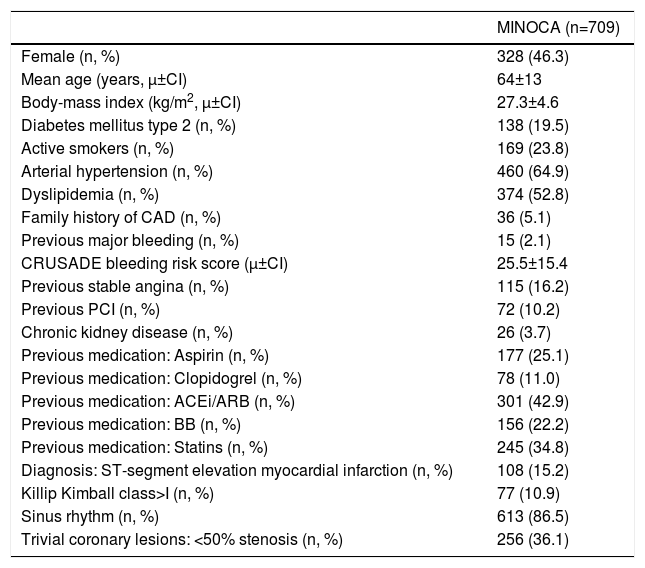
ResultsOf the 16 237 patients included in the registry, 709 (4.4%) were classified as MINOCA. Clinical baseline characteristics are described in Table 1.
Baseline characteristics.
| MINOCA (n=709) | |
|---|---|
| Female (n, %) | 328 (46.3) |
| Mean age (years, μ±CI) | 64±13 |
| Body-mass index (kg/m2, μ±CI) | 27.3±4.6 |
| Diabetes mellitus type 2 (n, %) | 138 (19.5) |
| Active smokers (n, %) | 169 (23.8) |
| Arterial hypertension (n, %) | 460 (64.9) |
| Dyslipidemia (n, %) | 374 (52.8) |
| Family history of CAD (n, %) | 36 (5.1) |
| Previous major bleeding (n, %) | 15 (2.1) |
| CRUSADE bleeding risk score (μ±CI) | 25.5±15.4 |
| Previous stable angina (n, %) | 115 (16.2) |
| Previous PCI (n, %) | 72 (10.2) |
| Chronic kidney disease (n, %) | 26 (3.7) |
| Previous medication: Aspirin (n, %) | 177 (25.1) |
| Previous medication: Clopidogrel (n, %) | 78 (11.0) |
| Previous medication: ACEi/ARB (n, %) | 301 (42.9) |
| Previous medication: BB (n, %) | 156 (22.2) |
| Previous medication: Statins (n, %) | 245 (34.8) |
| Diagnosis: ST-segment elevation myocardial infarction (n, %) | 108 (15.2) |
| Killip Kimball class>I (n, %) | 77 (10.9) |
| Sinus rhythm (n, %) | 613 (86.5) |
| Trivial coronary lesions: <50% stenosis (n, %) | 256 (36.1) |
ACEi: angiotensin converter enzyme inhibitors; ARB: angiotensin receptor blocker; BB: beta blockers; CAD: coronary artery disease; CI: confidence interval; MINOCA: myocardial infarction with non-obstructive coronary artery disease; PCI: percutaneous coronary intervention.
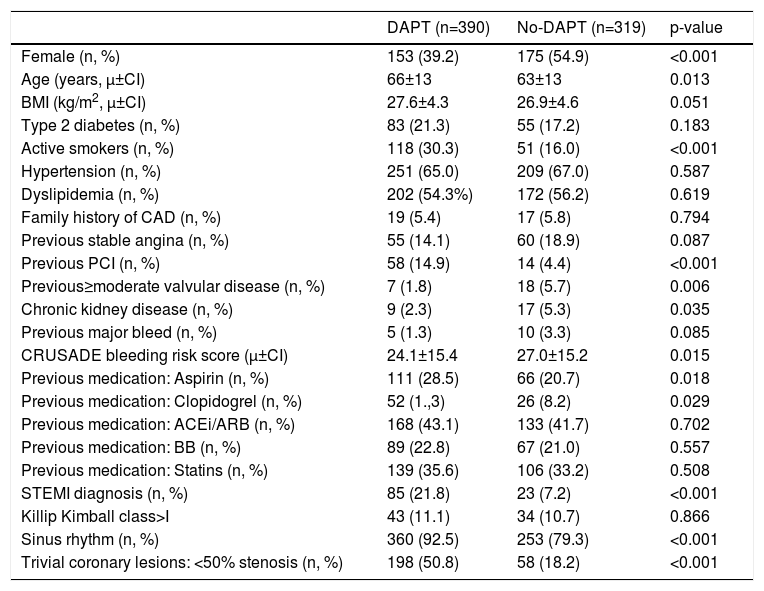
At discharge, DAPT was prescribed to 55.0% (n=390) of patients. Univariate comparison of both DAPT and non-DAPT groups is presented in Table 2.
Univariate comparison by study group.
| DAPT (n=390) | No-DAPT (n=319) | p-value | |
|---|---|---|---|
| Female (n, %) | 153 (39.2) | 175 (54.9) | <0.001 |
| Age (years, μ±CI) | 66±13 | 63±13 | 0.013 |
| BMI (kg/m2, μ±CI) | 27.6±4.3 | 26.9±4.6 | 0.051 |
| Type 2 diabetes (n, %) | 83 (21.3) | 55 (17.2) | 0.183 |
| Active smokers (n, %) | 118 (30.3) | 51 (16.0) | <0.001 |
| Hypertension (n, %) | 251 (65.0) | 209 (67.0) | 0.587 |
| Dyslipidemia (n, %) | 202 (54.3%) | 172 (56.2) | 0.619 |
| Family history of CAD (n, %) | 19 (5.4) | 17 (5.8) | 0.794 |
| Previous stable angina (n, %) | 55 (14.1) | 60 (18.9) | 0.087 |
| Previous PCI (n, %) | 58 (14.9) | 14 (4.4) | <0.001 |
| Previous≥moderate valvular disease (n, %) | 7 (1.8) | 18 (5.7) | 0.006 |
| Chronic kidney disease (n, %) | 9 (2.3) | 17 (5.3) | 0.035 |
| Previous major bleed (n, %) | 5 (1.3) | 10 (3.3) | 0.085 |
| CRUSADE bleeding risk score (μ±CI) | 24.1±15.4 | 27.0±15.2 | 0.015 |
| Previous medication: Aspirin (n, %) | 111 (28.5) | 66 (20.7) | 0.018 |
| Previous medication: Clopidogrel (n, %) | 52 (1.,3) | 26 (8.2) | 0.029 |
| Previous medication: ACEi/ARB (n, %) | 168 (43.1) | 133 (41.7) | 0.702 |
| Previous medication: BB (n, %) | 89 (22.8) | 67 (21.0) | 0.557 |
| Previous medication: Statins (n, %) | 139 (35.6) | 106 (33.2) | 0.508 |
| STEMI diagnosis (n, %) | 85 (21.8) | 23 (7.2) | <0.001 |
| Killip Kimball class>I | 43 (11.1) | 34 (10.7) | 0.866 |
| Sinus rhythm (n, %) | 360 (92.5) | 253 (79.3) | <0.001 |
| Trivial coronary lesions: <50% stenosis (n, %) | 198 (50.8) | 58 (18.2) | <0.001 |
ACEi: angiotensin converter enzyme inhibitors; ARB: angiotensin receptor blocker; BB: beta blockers; BMI: body mass index; CAD: coronary artery disease; CI: confidence level; DAPT: dual antiplatelet therapy; PCI: percutaneous coronary intervention; STEMI: ST elevated myocardial infarction.
DAPT group patients were older (66±13 vs. 63±13, p=0.013), had fewer female patients (39.2% vs. 54.9%, p<0.001) and more active smokers (30.3% vs. 16.0%, p<0.001). Previous percutaneous coronary intervention (PCI), 14.9% vs. 4.4%, p<0.001), aspirin (28.5% vs. 20.7%, p=0.018) or clopidogrel (13.3% vs. 8.2%, p=0.029) were more prevalent in the DAPT group. At admission, patients discharged on DAPT had higher ST elevation MI diagnosis (STEMI) (19.7% vs. 9.7%, p<0.001), sinus rhythm (92.5% vs. 79.3%, p<0.001) and trivial coronary lesions on coronary angiography (50.8% vs. 18.2%, p<0.001). The presence of at least moderate valvular heart disease was more frequent in the non-DAPT group (5.7% vs. 1.8%, p=0.006). In a univariate comparison, the baseline CRUSADE bleeding risk score was higher in the MINOCA patients that were discharged without DAPT (27.0±15.2 vs. 24.1±15.4 p=0.015).
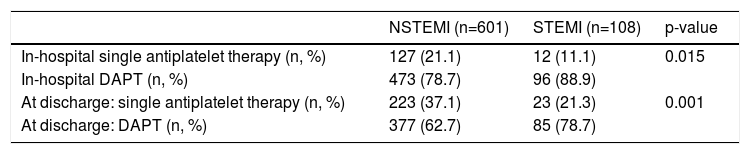
A comparison of the in-hospital and at discharge antiplatelet strategy between STEMI and non-STMI patients is presented in Table 3; in both situations, there was a higher prevalence of DAPT prescription in STEMI patients.
Antiplatelet strategy according to type of myocardial infarction.
| NSTEMI (n=601) | STEMI (n=108) | p-value | |
|---|---|---|---|
| In-hospital single antiplatelet therapy (n, %) | 127 (21.1) | 12 (11.1) | 0.015 |
| In-hospital DAPT (n, %) | 473 (78.7) | 96 (88.9) | |
| At discharge: single antiplatelet therapy (n, %) | 223 (37.1) | 23 (21.3) | 0.001 |
| At discharge: DAPT (n, %) | 377 (62.7) | 85 (78.7) |
DAPT: dual antiplatelet therapy; NSTEMI: non-ST elevated myocardial infarction; STEMI: ST elevated myocardial infarction.
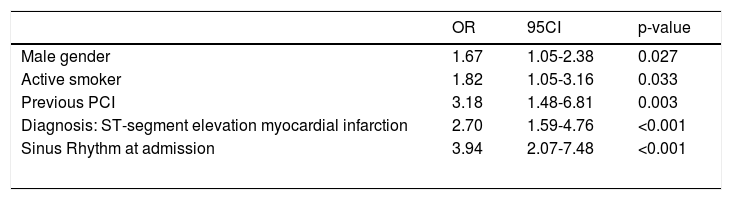
After multivariate analysis, independent predictors of DAPT use were identified (Table 4). The Hosmer-Lemeshow test showed good calibration for this model (p=0.998).
Multivariate analysis for DAPT independent use predictors.
| OR | 95CI | p-value | |
|---|---|---|---|
| Male gender | 1.67 | 1.05-2.38 | 0.027 |
| Active smoker | 1.82 | 1.05-3.16 | 0.033 |
| Previous PCI | 3.18 | 1.48-6.81 | 0.003 |
| Diagnosis: ST-segment elevation myocardial infarction | 2.70 | 1.59-4.76 | <0.001 |
| Sinus Rhythm at admission | 3.94 | 2.07-7.48 | <0.001 |
DAPT: dual antiplatelet therapy; PCI: percutaneous coronary intervention.
In this nationwide trial which included 709 MINOCA patients, DAPT was prescribed at discharge to 55.0% (n=390) of subjects. This is the first trial specifically studying the Portuguese prescription pattern in MINOCA patients and one of the largest currently published trials regarding MINOCA. A trial by Paolisso et al., which included 134 MINOCA patients, identified a 42.1% rate for DAPT prescription at discharge,10 while analysis by the SWEDEHEART registry indicates a 66.4% rate of DAPT prescription at discharge.6 Our results thus corroborate previously published data. The explanation for this rate of DAPT in patients with non-obstructive CAD is, however, not clear. As a working diagnosis, MINOCA represents a heterogeneous group of patients,11 making specific therapy difficult. Underlying etiologies include some clinical scenarios in which any degree of antithrombotic treatment could be recommended (such as plaque erosion, coronary embolism, missed ostial coronary occlusion, coronary artery dissection, pulmonary embolism or thrombophilia),3,12 but other causes may also be present (myocarditis, Takotsubo cardiomyopathy, and cardiac trauma, for example).3,13 In our trial, we believe that since the ProACS registry does not include patients in whom myocarditis or Takotsubo cardiomyopathy is the first suspected diagnosis, its prevalence as the underlying etiology may be lower than in other trials.4,13,14 Hence, the remaining MINOCA causes may include a proportionally higher rate of situations for which DAPT is thought to have a beneficial impact. Overall, and according to the baseline data presented (Tables 1 and 2), few MINOCA patients had a previous major bleeding event (n=15, 2.1%). Despite the CRUSADE bleeding risk score being lower in patients that were discharged under DAPT, both values represent a low risk status (corresponding to a mean bleeding risk score ≤5%).15,16 Also, after multivariate analysis, bleeding risk was not an independent predictor of DAPT use. Beyond sinus rhythm, the other variables presented as independent predictors identify groups of patients who are usually thought of as more prone to thrombus formation and pro-thrombotic events. There was a higher prevalence of DAPT prescription both in-hospital and at discharge in STEMI patients which has already been described in patients with obstructive CAD.17 Non-sinus rhythm patients include those who clearly benefit from anticoagulation,18 and DAPT use would increase their bleeding risk significantly.18 Studies of intracoronary imaging have shown that nearly 40% of patients with MINOCA have some evidence of plaque disruption,19 where DAPT may be useful.20 A recent study using optical coherence tomography and cardiac magnetic resonance (CMR) in 38 consecutive MINOCA patients identified plaque disruption in 24% and thrombus in 18% of the studied coronary arteries, in a total of 11 (28.9%) patients.21
This analysis of the ProACS registry, which included more than 17 000 patients, indicated a 4.4% prevalence of MINOCA. There is a substantial variability in reported prevalence of MINOCA, according to definitions applied and to the baseline population studied, with a range of 3.5 to 15%.3,4,10,12,13,22 Hence, the prevalence presented herein is in-line with the previously published data, with the exception of a predominance of male subjects. With regard to baseline characteristics, our population presents a similar prevalence of cardiovascular risk factors to other MINOCA populations described in the literature.4,23 STEMI was diagnosed in 15.2% of patients, similar to the data presented in the SWEDEHEART registry analysis (17%).6
Regarding limitations, the final etiological diagnosis was not considered in the ProACS registry. One particular concern is about the unknown use of CMR to reach a final diagnosis.24 However, our aim was to identify in which MINOCA patients DAPT is currently used, in both undiagnosed and during diagnostic work-up patients – where CMR is essential. In fact, recent authors have recommended the exclusion of myocarditis before establishing a MINOCA diagnosis work-up, since it is a highly frequent cause of chest pain and troponin elevation without CAD and has an established therapeutic approach and known prognosis.4,25 However, as previously mentioned, the ProACS registry excludes all patients in whom myocarditis is the main suspected diagnosis, limiting the impact of this factor in our analysis. Other limitations include the fact that coronary angiography was not routinely reviewed to search for missing stenosis or coronary artery dissection. Data obtained from intracoronary imaging studies is not available in the ProACS registry. The addition of intravascular imaging could provide interesting data regarding other diagnoses, especially non-obstructive plaque thrombosis and coronary artery dissection, as previous trials have proven.22,26 Finally, at the time of this analysis, no follow-up data was available for these patients, therefore, it was not possible to assess the incidence of bleeding according to the antithrombotic therapy used. The ProACS registry does not include all Portuguese centers managing patients with ACS, thus national prevalence of MINOCA may be underrepresented. Even when appropriately diagnosed, the management of MINOCA patients will vary depending on local practices and hospital resources.14 However, few nationwide registries have higher levels of representativeness:27 the ProACS registry is currently only surpassed by the SWEDEHEART and the MINAP registries,28,29 and the SWEDEHEART registry presents a published MINOCA rate of 8%.6
Since DAPT had a neutral effect in the only single trial to date addressing secondary MINOCA prevention,6 the results herein presented highlight the need to perform a thorough etiological study in all MINOCA patients. The authors believe that the group of MINOCA patients discharged on DAPT represent those in whom clinicians currently believe DAPT should be of benefit, either during the time needed to achieve a final underlying diagnosis or in those in whom a final diagnosis is never achieved. Future trials on MINOCA therapy (such as the MINOCA-BAT, ClinicalTrials.gov identifier 03686696) will be helpful to understand which therapeutic measures we should follow for these patients.
ConclusionThe results of this nationwide registry analysis indicate that 4.4% of patients with a diagnosis of MI had no significant CAD and that the majority (55%) of these patients were discharged on DAPT. Male patients, active smokers, the presence of sinus rhythm at admission, a STEMI diagnosis and a previous history of PCI were independent predictors of DAPT use. The issue of how to handle antithrombotic agents in MINOCA patients is a topic open for discussion and requires additional investigation.
Conflicts of interestThe authors have no conflicts of interest to declare.
