


Cardiac tumors in the pediatric population are rare, their incidence range between 0.001% and 0.003%. They are mostly benign, rhabdomyomas the most common type, followed by fibromas. The clinical features are being usually nonspecific and depend on the size and location of the tumor within the heart.
We report the case of a previously healthy four-year-old boy referred for flu-like symptoms. A respiratory infection was suspected and a chest X-ray showed an increased cardiothoracic index. An echocardiogram revealed a single large heterogeneous mass in the left ventricle emerging from the lateral wall. Despite its size, the mass did not obstruct the left ventricular outflow tract or affect mitral valve function. Cardiac magnetic resonance imaging showed a large mass whose imaging features were suggestive of a fibroma. He became symptomatic during follow-up and was referred for surgical excision of the mass. Histological study confirmed a fibroma. At present the patient remains asymptomatic.
Os tumores cardíacos são uma entidade rara em idades pediátricas, com uma incidência variável entre 0,001% e 0,003%. Sendo habitualmente benignos, os rabdomiomas e os fibromas são os tipos histológicos mais frequentes. A clínica é inespecífica e dependente das dimensões e localização do tumor.
Descreve-se o caso de uma criança de quatro anos previamente saudável e assintomática, observada em contexto de infecção respiratória, tendo-se identificado cardiomegália na teleradiografia torácica. A ecocardiografia transtorácica revelou uma massa volumosa e heterogénea no ventrículo esquerdo, sem causar obstrução da câmara de saída ou disfunção valvular. A ressonância magnética foi sugestiva de fibroma. Procedeu-se a terapêutica cirúrgica, com excisão completa que confirmou fibroma mantendo-se assintomática.
Primary cardiac tumors in the pediatric population are mostly benign, rhabdomyoma being the most common type, followed by fibroma, myxoma and teratoma1-6.
The clinical features are usually nonspecific and depend on the size and location of the tumor; they can include precordialgia, general symptoms of fever and asthenia, arrhythmias or signs of low cardiac output due to outflow tract obstruction. Diagnosis is accordingly often not made until serious complications arise, such as pericardial effusion or tamponade, embolic events, syncope or sudden death, which can occur even in previously asymptomatic cases1,2.
Case reportWe report the case of a previously healthy four-year-old boy, who was seen in the emergency department of his local hospital with odynophagia, fever and productive cough, of three days' evolution. He had no symptoms of fatigue, asthenia, palpitations, exertional dyspnea, orthopnea, or episodes of fainting or syncope.
Cardiopulmonary auscultation revealed a low-frequency grade II/IV systolic murmur at the left sternal border. No other alterations were observed on physical examination, including adventitious lung sounds, abnormal vital signs, jugular distension or hepatojugular reflux. Since a respiratory infection was suspected, a chest X-ray was performed, which showed an increased cardiothoracic index (62%) with left-sided cardiomegaly, but no pulmonary abnormalities, and the patient was referred to our department for observation.
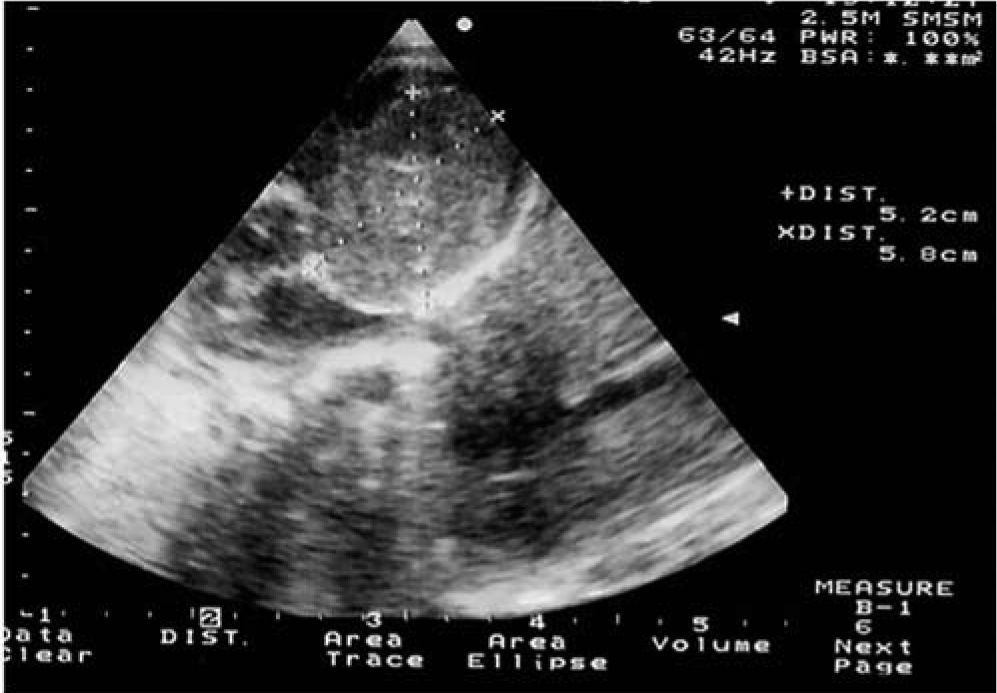
Laboratory tests (blood count, biochemical screen, coagulation profile and tumor markers) revealed no abnormalities. A 12-lead electrocardiogram (ECG) showed sinus rhythm with left axis deviation of the QRS complex and left anterior hemiblock. Transthoracic echocardiography revealed a large heterogeneous mass in the left ventricle emerging from the free wall (Figure 1). Despite its size, the mass did not obstruct the left ventricular outflow tract or affect mitral valve function. No other abnormalities were observed on the echocardiogram.
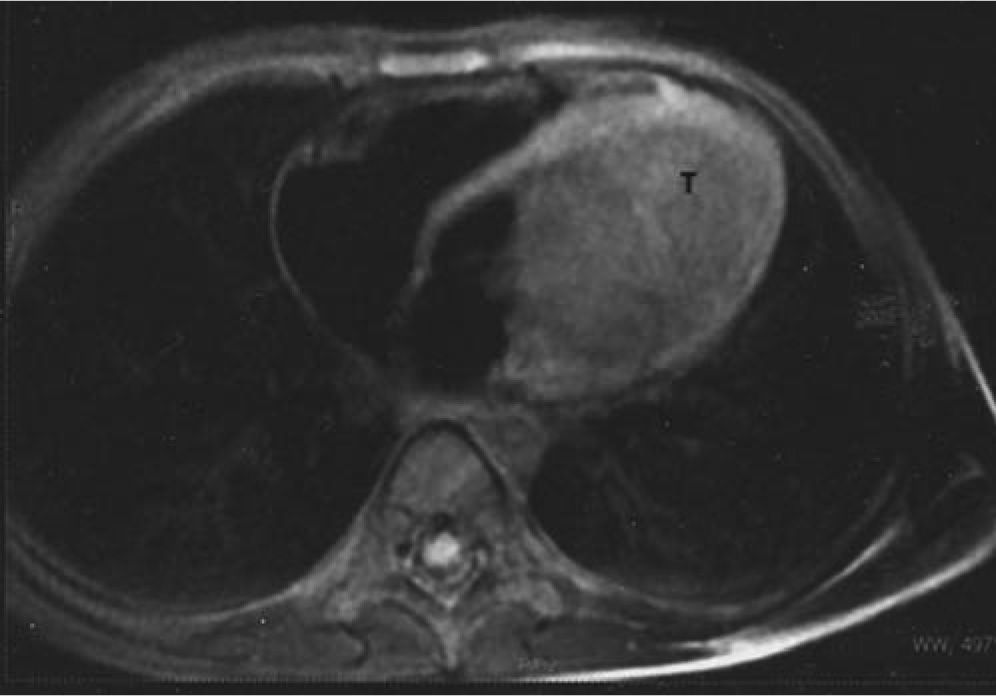
For more detailed characterization of the ventricular mass, cardiac magnetic resonance imaging was performed, which confirmed the presence of a large structure, of solid appearance, emerging from the upper wall of the left ventricle and protruding slightly into the outflow tract (Figure 2). The mass, measuring 5.5×4.5cm, presented a homogeneous signal in all sequences, including delayed enhancement study. It was thus considered likely to be a myocardial fibroma.
Fainting episodes at rest were reported during follow-up. Serial ECGs and 24-hour Holter monitoring showed no ventricular arrhythmias or signs of myocardial ischemia. The patient underwent surgical treatment at a referral hospital abroad, by left ventriculotomy (pericardiotomy and myocardiotomy with preservation of the endocardium) with complete macroscopic excision of the mass, with no complications.
Postoperative echocardiography showed excellent function, with no left ventricular outflow tract obstruction.
The patient was discharged seven days after the operation. Histological study confirmed a fibroma. He has remained asymptomatic during follow-up, echocardiography showing slight dyskinesia of the ventricular wall at the excision site, with no signs of recurrence of the tumor.
DiscussionCardiac tumors, both primary and secondary, are rare in the pediatric population. Their incidence ranges between 0.001% and 0.003%3, with a similar distribution between the sexes. Unlike in adults, the most common histological type is rhabdomyoma, which accounts for 60% of benign primary cardiac tumors in children aged under 12 months. In children aged 1–15 years, rhabdomyoma accounts for 41% and fibroma 14% of benign cardiac tumors1–3. Fibromas usually occur in the left ventricle, presenting as a single lesion of variable size, and may have calcifications or areas of intratumoral necrosis.
Due to the nonspecific nature of symptoms, many are diagnosed following an echocardiographic finding, as in the case presented4–6. Cardiac magnetic resonance imaging provides morphological characterization of some cardiac tumors, such as fibromas and myxomas, as well as assessment of the extent of myocardial, pericardial and extracardiac involvement7.
Surgical treatment is indicated in cases of ventricular arrhythmia refractory to medical therapy, inflow and/or outflow tract obstruction, or heart failure. If surgical resection is not possible, heart transplantation should be considered.
Conflicts of interestThe authors have no conflicts of interest to declare.
