
Atrial fibrillation (AF) is the most common sustained arrhythmia in clinical practice and a major cause of morbidity, due to the associated risk of stroke. However, since it is often paroxysmal, it is commonly underdiagnosed and undertreated.
ObjectivesThe primary objective of this prospective study was to determine the prevalence of paroxysmal atrial fibrillation (PAF) in patients aged 40 and above in a population who underwent continuous 24-hour electrocardiographic monitoring. The secondary objectives were to determine the overall prevalence of AF/atrial flutter (AFL) regardless of the type and to compare the population with AF with the general population and patients with PAF with patients with AF.
ResultsA total of 4843 consecutive patients were analyzed, 58% women, 26.2% aged 70-79 years (n=1269), 25.9% (n=1252) aged 60-69 years, and 19.0% (n=923) aged 50-59 years; the others were aged either >80 years (n=712, 14.7%) or <50 years (n=686, 14.2%). At least one episode of PAF was detected in 123 patients, a prevalence of 2.5% (95% CI: 2.1-3.0). The prevalence of persistent AF throughout the monitoring period was 9.4% (95% CI: 8.6-10.2) (n=454). Additionally, 39 cases of typical AFL were detected, but in 23 of them (sustained or paroxysmal) this appeared isolated, a prevalence of 0.8% (95% CI: 0.6-1.1). The overall prevalence of AF/AFL was thus 12.4%. The presence of some type of AF/AFL was significantly correlated with male gender (p<0.001), age (especially in the 70-79 and >80 age-groups) (p<0.001) and hypertension (p<0.001). This group had a significantly higher prevalence of previous stroke (56 patients [9.3%], p=0.001) and acute myocardial infarction (5.3%, p<0.001). Comparing the population with PAF and/or paroxysmal AFL (PAF/PAFL) to those with persistent AF (during 24-hour monitoring), significant differences were found: a higher prevalence of PAF/PAFL in younger individuals (40-49, 50-59 and 60-69 age-groups) and lower in older individuals (70-79 and >80 age-groups) (p<0.001), higher prevalence of history of stroke (p=0.024), and lower levels of hypertension (p<0.001). Only 12.8% of patients with PAF were taking anticoagulant drugs.
ConclusionsThe prevalence of PAF found in a population referred for continuous 24-hour electrocardiographic monitoring for diverse reasons was 2.5% and the overall AF/AFL prevalence was 12.4%. PAF was more prevalent in younger patients. Patients with PAF showed a significantly lower prevalence of hypertension and significantly higher rates of stroke. Systematically detecting patients with PAF is a major public health concern, since early diagnosis is essential to identify candidates for oral anticoagulation and catheter ablation, which is frequently curative when applied at this stage.
A fibrilhação auricular (FA) é a arritmia sustentada mais frequente na prática clínica, constituindo uma importante causa de morbilidade pelo risco associado de acidente vascular cerebral (AVC). Devido ao seu caráter muitas vezes paroxístico encontra-se, contudo, subdiagnosticada e subtratada.
ObjetivosEstudo prospetivo que tem como objetivo principal o cálculo da prevalência da FA paroxística em doentes com 40 ou mais anos de idade, numa população submetida a monitorização eletrocardiográfica contínua de 24 horas. Como objetivos secundários: o cálculo da prevalência total de FA e flutter auricular (FLA), independentemente do tipo, e a comparação entre as populações com FA versus população total e FA paroxística versus FA persistente nas 24 horas.
ResultadosEste estudo analisou um total de 4843 doentes consecutivos, 58% dos quais do sexo feminino. Vinte seis vírgula dois por cento dos doentes encontrava-se na faixa etária dos 70-79 anos (n=1269), 25,9% (n-1252) entre os 60-69 anos e 19,0% (n-923) entre os 50-59 anos; os restantes doentes ou tinham idades superiores a 80 anos (n=712, 14,7%), ou inferiores a 50 (n=686, 14,2%). Entre os doentes referenciados e analisados, registaram-se 123 com registo de pelo menos um período de FA paroxística, o que equivale a uma prevalência de 2,5% (IC a 95%, 2,1-3,0). A prevalência de doentes com FA durante todo o registo foi de 9,4% (IC a 95%, 8,6-10,2) (n=454). Registaram-se ainda 39 casos de doentes com flutter típico, mas em 23 quer mantido quer paroxístico aparecia isolado, o que corresponde a uma prevalência de 0,8% (IC a 95%, 0,6 a 1,1). Tal indica que a prevalência de doentes com FA/FL total é de 12,4%. A presença de alguma forma de FA/FLA correlacionou-se significativamente com sexo masculino (p<0,001) e idade (sobretudo nas classes etárias dos 70-79 anos e>80 anos) (p<0,001), com hipertensão arterial (p<0,001). Este grupo tem uma prevalência significativamente maior de antecedentes de AVC (p=0,001), 56 pacientes (9,3%), bem como de enfarte agudo do miocárdio, 5,3% (p<0,001). Ao comparar a população de doentes com FA paroxística e FLA paroxístico (FA/FLp) versus FA persistente, verificaram-se diferenças significativas (p<0,05) entre ambos nos seguintes parâmetros: prevalência significativamente maior de FA/FLp nos indivíduos situados nas classes etárias mais jovens (entre os 40-49, 50-59 e 60-69 anos), e significativamente menor nos indivíduos situados nas classes etárias dos 70-79 anos e>80 anos (p<0,001); prevalência significativamente maior de antecedentes de AVC (p=0,024) e significativamente menor de hipertensão arterial (p<0,001). Apenas 12,8% dos que apresentavam FA paroxística estavam hipocoagulados.
ConclusõesA prevalência da FA paroxística encontrada numa população submetida por motivos não selecionados a monitorização eletrocardiográfica de 24 horas é de 2,5% e a prevalência total de FA/FLA é de 12,4%. A FA paroxística afeta doentes mais jovens, sendo menos dependente de fatores de risco, como hipertensão arterial. Correlaciona-se com percentagens significativamente superiores de AVC. A deteção sistemática destes doentes é um importante problema de saúde pública sendo diagnóstico precoce essencial na definição de candidatos para hipocoagulação oral e tratamento por ablação por cateter, a qual apresenta uma elevada taxa de sucesso curativa quando aplicada nesta fase.
Atrial fibrillation (AF) is the most common sustained arrhythmia in clinical practice, with an incidence of 19.2 per 1000 person/years in individuals aged over 65 years. It is a major cause of morbidity due to the condition itself and to the associated risk of thromboembolic stroke, and has been shown to be an independent risk factor for both overall mortality and sudden cardiac death.1
In the Framingham study, the annual risk for stroke attributable to AF was 1.5% in patients aged 50-59 years, rising steeply to 23.5% in those aged over 80.2
The incidence of stroke and associated mortality are higher in Portugal than in most European countries. The annual stroke incidence may be as high as 3.05 per 1000 population in rural areas of northern Portugal and 2.69 in the Greater Porto urban area. These figures are higher than the European average and cannot be attributed solely to other known risk factors for stroke.3
One possible explanation could be that AF is also more prevalent in the Portuguese population. This was the rationale for the FAMA study,4 which included 10447 individuals aged 40 and over of both genders and from all areas of the country. This epidemiological survey found an overall AF prevalence of 2.5%, which was much higher in those aged 70-79 years (6.6%) and in those aged 80 or over (10.4%). Prevalence was, however, low in younger individuals (1.6% for those aged 60-69 years). In the FAMA study, AF was diagnosed by 12-lead electrocardiogram (ECG) and the study sample was selected by random home visits throughout the country.
The prevalence found in the FAMA study was higher than expected considering the results of previous studies in the Portuguese population but lower than in studies in other European countries that served as a reference for it.5 For instance, in the Rotterdam study, which ran from 1990 to 2000 and included 7983 subjects aged 55 years and above (mean age 69.3 years) assessed by 12-lead ECG, baseline assessment indicated an overall prevalence of 5.5%.5 Based on the results of this study and the gender and age distribution of the Portuguese population in 2009, the prevalence of AF could be estimated at around 3.8% for those aged 45 or more and 6.8% for those aged over 60. This discrepancy could be due to the fact that the sample in the Rotterdam study was confined to a small geographical area, while the FAMA study included a much wider population.
One limitation of the FAMA study4 is the fact that heart rhythm was only assessed during a short ECG reading, which will inevitably lead to underestimation of the prevalence of AF if it is paroxysmal. On the basis of the study's results, it became clear that AF is underdiagnosed and undertreated, especially since a non-systematic analysis of clinical practice suggests that paroxysmal AF (PAF) is at least three times as common as persistent AF. There are in fact few estimates of the prevalence of PAF – around 50% in the Framingham study3,4 and 35-60% in other studies – and these refer mainly to symptomatic forms.
Holter 24-hour continuous ECG monitoring is routinely used to assess various symptoms, especially palpitations. It is commonly used to determine the heart rate profile in patients with known AF and to assess the effectiveness of antiarrhythmics or catheter ablation in maintaining sinus rhythm.
Although Holter monitoring is undoubtedly better than 12-lead ECG for assessing the prevalence of AF, since it can identify paroxysmal episodes that would not otherwise be detected, it still estimates prevalence by default. Furthermore, it cannot distinguish with certainty between persistent and long-standing persistent AF, which are considered distinct entities in the ESC guidelines for the management of AF.6 The definition of PAF – AF lasting less than 48 hours – also means that monitoring for only 24 hours may diagnose what is actually PAF as persistent AF.
Nevertheless, the fact that Holter monitoring provides longer ECG recordings means that it enables a more thorough assessment of AF prevalence, identifying individuals with daily paroxysmal episodes who are as vulnerable to thromboembolism as those with sustained AF and a similar risk profile.
The method used in this study, 12-lead Holter monitoring, has advantages over the more common 3-lead Holter, offering a more precise analysis of the patient's rhythm patterns than a conventional 12-lead ECG, with the additional benefit of identifying the onset and end of the episode, transitions between AF and atrial flutter (AFL), and episodes of atrial tachycardia, a condition that is often confused with AF.
The same definitions of AF and AFL can be used for 12-lead Holter monitoring as for the conventional ECG. AF is defined as an arrhythmia with continuous irregular R-R intervals and randomly oscillating baseline with absence of P waves. The most common form of AFL, designated typical AFL, is characterized by predominantly negative biphasic F waves in the inferior leads with a sawtooth pattern and predominantly positive F waves in V1. AFL is termed atypical if the F-wave morphology is different from the common type.7
Holter study is frequently performed routinely, often as part of a cardiological assessment. Individuals who are referred for Holter monitoring by their general practitioner (GP) are fairly typical of the general population, since the reasons for referral are diverse; this reduces selection bias and makes this population a suitable basis for a study estimating AF prevalence which is more likely to give valid conclusions that can be extrapolated to the general population.
The present study aims to determine the prevalence of PAF and, on the basis of its results, to contribute to the development of strategies for the prevention and treatment of AF in Portugal.
ObjectivesThe primary objective of this prospective study was to determine the prevalence of PAF in patients aged 40 and above.
The secondary objectives were to determine the overall prevalence of AF/AFL regardless of the type and to compare the population with AF with the general population and patients with PAF with patients with persistent AF, in a population who underwent continuous 24-hour electrocardiographic monitoring.
MethodsThis was a prospective cross-sectional epidemiological study of individuals referred for Holter study in two reference centers covering the Douro Litoral and Beira Litoral geographic areas, which include all of the Greater Porto urban area.
The individuals under study, who had contacted one of these centers after being referred by their GP for 24-hour Holter monitoring, were assessed and included in the study population regardless of the reason for referral. Patients of both sexes aged 40 and above who had undergone continuous 12-lead ECG monitoring for any reason in the participating centers during the study period and who provided written informed consent were included in the study. Individuals who did not for any reason fulfill the inclusion criteria at the time of the exam, or who refused to provide written consent, were excluded.
The Holter exams were performed by trained staff according to the same protocol and to the same quality standards in both participating centers, both private laboratories, using Mortara 12-lead recorders equipped with solid-state digital memory. Three arrhythmologists oversaw review and validation of the exam and the data were interpreted by two experienced cardiac technicians.
All participants completed a questionnaire providing information on demographics, clinical history, symptoms and medication.
The data were recorded by members of the study team in a dedicated database designed by Keypoint, Consultoria Científica, Lda, in which the Holter readings could be reviewed semi-automatically or manually by the three arrhythmologists, independently and blinded to all other patient data. The diagnosis was recorded in the database; if the assessments of the first two arrhythmologists differed, the third arrhythmologist was automatically notified in order to resolve the conflict.
AF was defined according to the standard ECG criteria described above. An episode of PAF was defined as one lasting longer than 30 s beginning and/or ending during the 24-hour recording, and persistent AF was defined as AF sustained throughout the 24-hour study.
The study was submitted to the National Data Protection Commission (CNPD) and to the Administrative Board of both centers before implementation.
Statistical analysisThe sample was defined in accordance with the study's primary objective, to determine the prevalence of PAF, assuming that this would be at least three times greater than the AF prevalence of 2.5% estimated by the FAMA study.
A total of 4843 patients were included, enabling 95% confidence intervals (CIs) to be estimated with a sampling error of ±1.0%.
A descriptive statistical analysis was performed of all study variables and 95% CIs were calculated for the estimated prevalences. Continuous variables were expressed as mean, median and standard deviation and categorical variables as absolute and relative frequencies.
The chi-square test was used to compare groups (patients with vs. without AF, and with PAF or AFL vs. with persistent AF) in terms of relative frequencies and the t test for independent samples was used to compare means, since all study variables had a normal distribution. The level of significance was taken to be p=0.05.
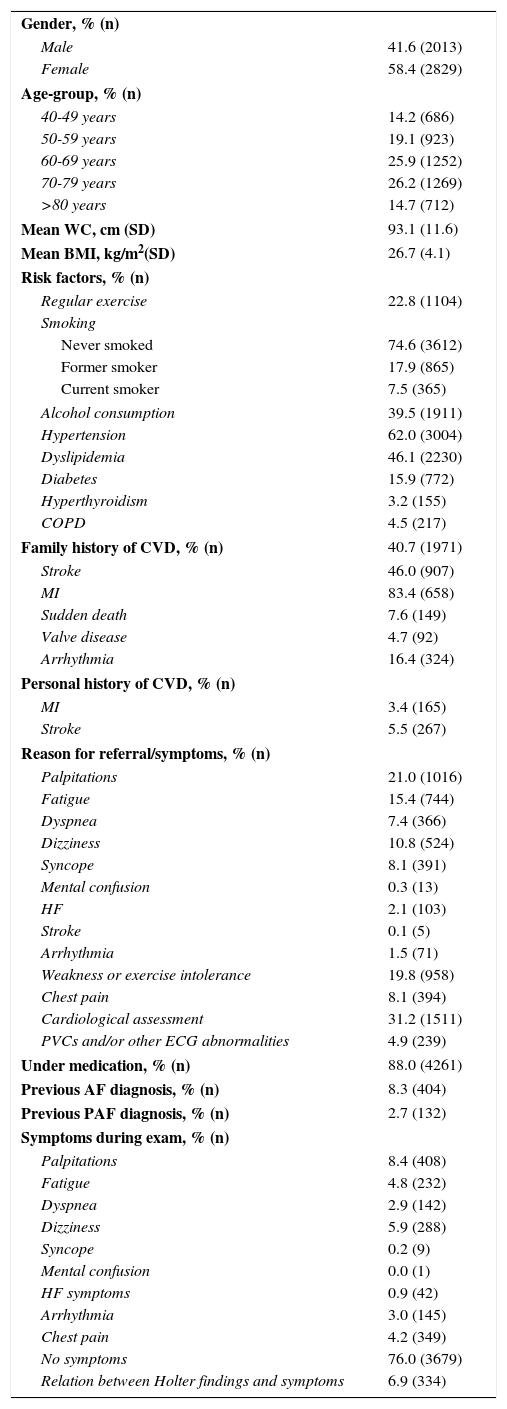
ResultsCharacteristics of the study populationOf the 4843 patients analyzed (Table 1), 58% were women, 26.2% were aged 70-79 years (n=1269), 25.9% (n=1252) aged 60-69 years, and 19.0% (n=923) aged 50-59 years; the others were aged either >80 years (n=712, 14.7%) or <50 years (n=686, 14.2%).
Characteristics of the study population.
| Gender, % (n) | |
| Male | 41.6 (2013) |
| Female | 58.4 (2829) |
| Age-group, % (n) | |
| 40-49 years | 14.2 (686) |
| 50-59 years | 19.1 (923) |
| 60-69 years | 25.9 (1252) |
| 70-79 years | 26.2 (1269) |
| >80 years | 14.7 (712) |
| Mean WC, cm (SD) | 93.1 (11.6) |
| Mean BMI, kg/m2(SD) | 26.7 (4.1) |
| Risk factors, % (n) | |
| Regular exercise | 22.8 (1104) |
| Smoking | |
| Never smoked | 74.6 (3612) |
| Former smoker | 17.9 (865) |
| Current smoker | 7.5 (365) |
| Alcohol consumption | 39.5 (1911) |
| Hypertension | 62.0 (3004) |
| Dyslipidemia | 46.1 (2230) |
| Diabetes | 15.9 (772) |
| Hyperthyroidism | 3.2 (155) |
| COPD | 4.5 (217) |
| Family history of CVD, % (n) | 40.7 (1971) |
| Stroke | 46.0 (907) |
| MI | 83.4 (658) |
| Sudden death | 7.6 (149) |
| Valve disease | 4.7 (92) |
| Arrhythmia | 16.4 (324) |
| Personal history of CVD, % (n) | |
| MI | 3.4 (165) |
| Stroke | 5.5 (267) |
| Reason for referral/symptoms, % (n) | |
| Palpitations | 21.0 (1016) |
| Fatigue | 15.4 (744) |
| Dyspnea | 7.4 (366) |
| Dizziness | 10.8 (524) |
| Syncope | 8.1 (391) |
| Mental confusion | 0.3 (13) |
| HF | 2.1 (103) |
| Stroke | 0.1 (5) |
| Arrhythmia | 1.5 (71) |
| Weakness or exercise intolerance | 19.8 (958) |
| Chest pain | 8.1 (394) |
| Cardiological assessment | 31.2 (1511) |
| PVCs and/or other ECG abnormalities | 4.9 (239) |
| Under medication, % (n) | 88.0 (4261) |
| Previous AF diagnosis, % (n) | 8.3 (404) |
| Previous PAF diagnosis, % (n) | 2.7 (132) |
| Symptoms during exam, % (n) | |
| Palpitations | 8.4 (408) |
| Fatigue | 4.8 (232) |
| Dyspnea | 2.9 (142) |
| Dizziness | 5.9 (288) |
| Syncope | 0.2 (9) |
| Mental confusion | 0.0 (1) |
| HF symptoms | 0.9 (42) |
| Arrhythmia | 3.0 (145) |
| Chest pain | 4.2 (349) |
| No symptoms | 76.0 (3679) |
| Relation between Holter findings and symptoms | 6.9 (334) |
AF: atrial fibrillation; BMI: body mass index; COPD: chronic obstructive pulmonary disease; CVD: cardiovascular disease; ECG: electrocardiographic; HF: heart failure; MI: myocardial infarction; PAF: paroxysmal atrial fibrillation; PVCs: premature ventricular contractions; SD: standard deviation; WC: waist circumference.
Analysis of risk factors showed that 62.0% of the study population had been diagnosed with hypertension, 46.1% with dyslipidemia, 15.9% with diabetes, 3.2% with hyperthyroidism, and 4.5% with chronic obstructive pulmonary disease (COPD).
Previous myocardial infarction (MI) was recorded in 3.5% (n=165) of the study population and previous stroke in 5.5% (n=267).
Most of the study population did not exercise regularly (77.2%, n=3.738), had never smoked (74.6%) and did not consume alcohol (60.5%).
Reasons for referral for Holter monitoring included palpitations (21.0%, n=1016), fatigue (15.4%, n=744), dyspnea (7.6%, n=366), dizziness (1.8%, n=524), syncope (8.1%, n=391), mental confusion (0.3%, n=13), weakness or exercise intolerance (19.8%, n=958), unspecified arrhythmia (1.5%, n=71), and chest pain (8.1%, n=394), as well as assessment of premature ventricular contractions (PVCs) and/or other ECG abnormalities (4.9%, n=239) and in the context of heart failure (HF) (2.1%, n=103) and previous stroke after the acute phase (0.1%, n=5). Referral was for unspecified clinical reasons, regardless of symptoms, in 1511 (31.2%) of cases.
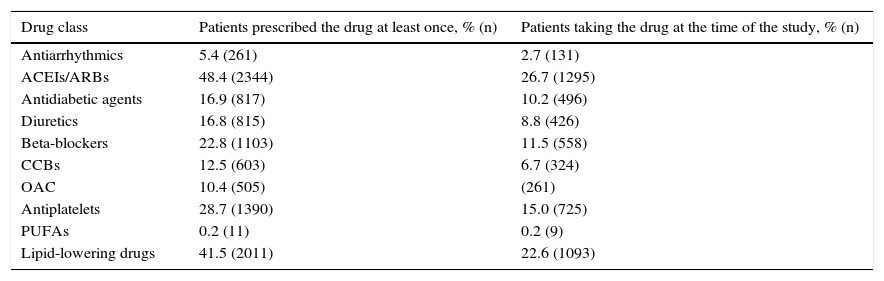
A total of 10 drug classes were used in the study population at some point: antiarrhythmics, angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs), antidiabetic agents, diuretics, beta-blockers, calcium channel blockers, polyunsaturated fatty acids, lipid-lowering drugs, antiplatelets and oral anticoagulants. Of these, ACEIs/ARBs were the most frequently prescribed (48.4%), followed by lipid-lowering drugs (41.5%), antiplatelets (28.7%) and beta-blockers (22.8%) (Table 2). Of medication used at the time of the study, ACEIs/ARBs were also the most frequently prescribed (26.7%), followed by lipid-lowering drugs (22.6%), antiplatelets (15.0%) and beta-blockers (11.5%). Oral anticoagulants had been prescribed at least once for 10.4% of patients and were currently being taken by 5.4%.
Medications used in the study population.
| Drug class | Patients prescribed the drug at least once, % (n) | Patients taking the drug at the time of the study, % (n) |
|---|---|---|
| Antiarrhythmics | 5.4 (261) | 2.7 (131) |
| ACEIs/ARBs | 48.4 (2344) | 26.7 (1295) |
| Antidiabetic agents | 16.9 (817) | 10.2 (496) |
| Diuretics | 16.8 (815) | 8.8 (426) |
| Beta-blockers | 22.8 (1103) | 11.5 (558) |
| CCBs | 12.5 (603) | 6.7 (324) |
| OAC | 10.4 (505) | (261) |
| Antiplatelets | 28.7 (1390) | 15.0 (725) |
| PUFAs | 0.2 (11) | 0.2 (9) |
| Lipid-lowering drugs | 41.5 (2011) | 22.6 (1093) |
ACEIs: angiotensin-converting enzyme inhibitors; ARBs: angiotensin receptor blockers; CCBs: calcium channel blockers; OAC: oral anticoagulants; PUFA: polyunsaturated fatty acids.
At least one episode of PAF was detected in 123 patients in a single 24-hour ECG recording, a prevalence of 2.5% (95% CI: 2.1-3.0%).
The proportion of patients with persistent AF (throughout the recording) was 9.4% (95% CI: 8.6-10.2%) (n=454).
Additionally, 39 cases of typical AFL were detected, 14 of whom also had PAF; in two PAF became regular, turning into AFL, but in 23 of them AFL was sustained or paroxysmal and appeared in isolation, a prevalence of 0.8% (95% CI: 0.6-1.1).
On the basis of these figures, the overall prevalence of persistent AF, PAF and/or isolated AFL in the study population was 12.4%.
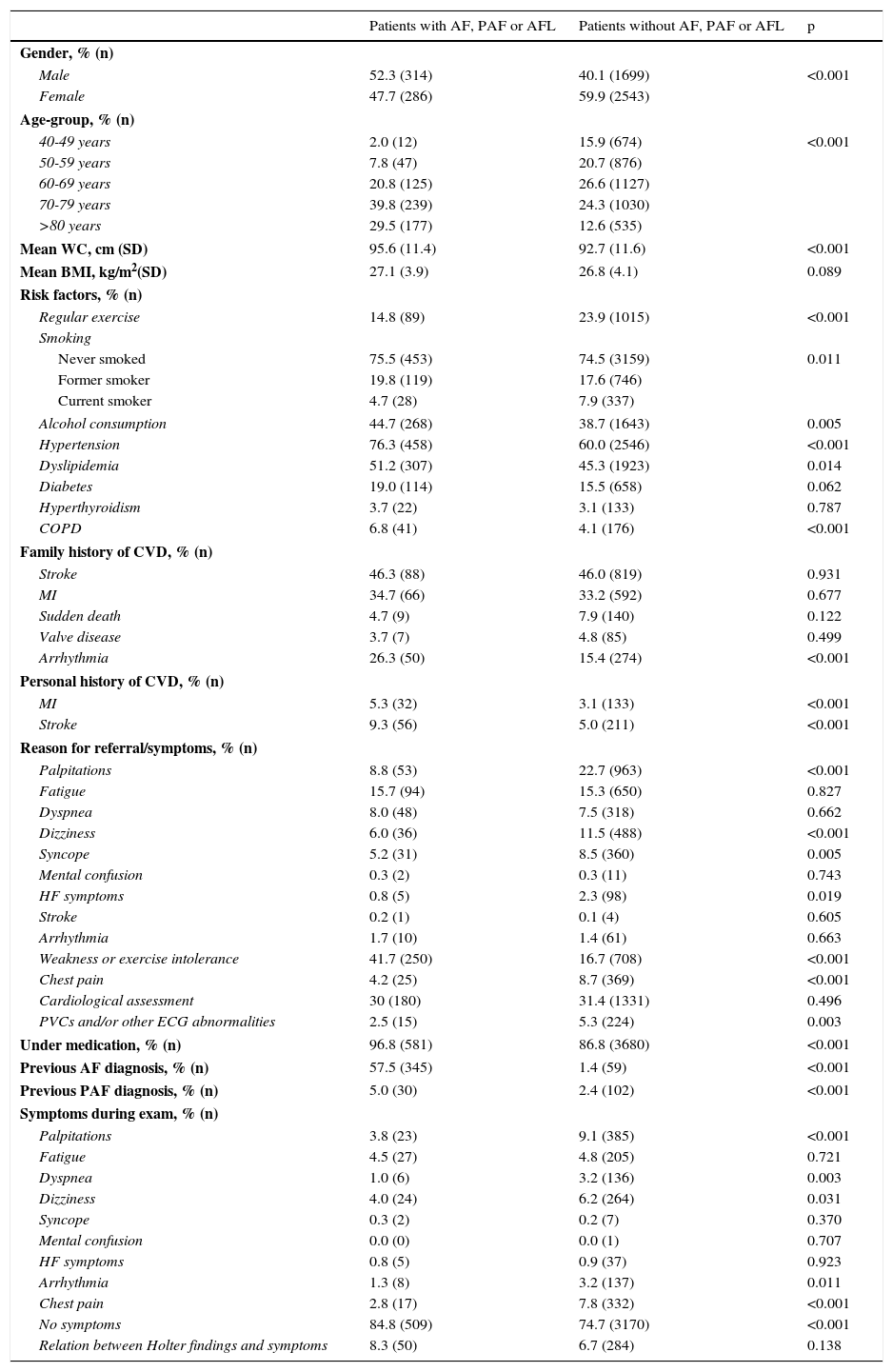
Characteristics of individuals with atrial fibrillation and comparison with those withoutTable 3 presents comparisons between individuals with any type of AF or AFL and those in sinus rhythm throughout the 24-hour monitoring period.
Characteristics of individuals with atrial fibrillation and comparison with those without.
| Patients with AF, PAF or AFL | Patients without AF, PAF or AFL | p | |
|---|---|---|---|
| Gender, % (n) | |||
| Male | 52.3 (314) | 40.1 (1699) | <0.001 |
| Female | 47.7 (286) | 59.9 (2543) | |
| Age-group, % (n) | |||
| 40-49 years | 2.0 (12) | 15.9 (674) | <0.001 |
| 50-59 years | 7.8 (47) | 20.7 (876) | |
| 60-69 years | 20.8 (125) | 26.6 (1127) | |
| 70-79 years | 39.8 (239) | 24.3 (1030) | |
| >80 years | 29.5 (177) | 12.6 (535) | |
| Mean WC, cm (SD) | 95.6 (11.4) | 92.7 (11.6) | <0.001 |
| Mean BMI, kg/m2(SD) | 27.1 (3.9) | 26.8 (4.1) | 0.089 |
| Risk factors, % (n) | |||
| Regular exercise | 14.8 (89) | 23.9 (1015) | <0.001 |
| Smoking | |||
| Never smoked | 75.5 (453) | 74.5 (3159) | 0.011 |
| Former smoker | 19.8 (119) | 17.6 (746) | |
| Current smoker | 4.7 (28) | 7.9 (337) | |
| Alcohol consumption | 44.7 (268) | 38.7 (1643) | 0.005 |
| Hypertension | 76.3 (458) | 60.0 (2546) | <0.001 |
| Dyslipidemia | 51.2 (307) | 45.3 (1923) | 0.014 |
| Diabetes | 19.0 (114) | 15.5 (658) | 0.062 |
| Hyperthyroidism | 3.7 (22) | 3.1 (133) | 0.787 |
| COPD | 6.8 (41) | 4.1 (176) | <0.001 |
| Family history of CVD, % (n) | |||
| Stroke | 46.3 (88) | 46.0 (819) | 0.931 |
| MI | 34.7 (66) | 33.2 (592) | 0.677 |
| Sudden death | 4.7 (9) | 7.9 (140) | 0.122 |
| Valve disease | 3.7 (7) | 4.8 (85) | 0.499 |
| Arrhythmia | 26.3 (50) | 15.4 (274) | <0.001 |
| Personal history of CVD, % (n) | |||
| MI | 5.3 (32) | 3.1 (133) | <0.001 |
| Stroke | 9.3 (56) | 5.0 (211) | <0.001 |
| Reason for referral/symptoms, % (n) | |||
| Palpitations | 8.8 (53) | 22.7 (963) | <0.001 |
| Fatigue | 15.7 (94) | 15.3 (650) | 0.827 |
| Dyspnea | 8.0 (48) | 7.5 (318) | 0.662 |
| Dizziness | 6.0 (36) | 11.5 (488) | <0.001 |
| Syncope | 5.2 (31) | 8.5 (360) | 0.005 |
| Mental confusion | 0.3 (2) | 0.3 (11) | 0.743 |
| HF symptoms | 0.8 (5) | 2.3 (98) | 0.019 |
| Stroke | 0.2 (1) | 0.1 (4) | 0.605 |
| Arrhythmia | 1.7 (10) | 1.4 (61) | 0.663 |
| Weakness or exercise intolerance | 41.7 (250) | 16.7 (708) | <0.001 |
| Chest pain | 4.2 (25) | 8.7 (369) | <0.001 |
| Cardiological assessment | 30 (180) | 31.4 (1331) | 0.496 |
| PVCs and/or other ECG abnormalities | 2.5 (15) | 5.3 (224) | 0.003 |
| Under medication, % (n) | 96.8 (581) | 86.8 (3680) | <0.001 |
| Previous AF diagnosis, % (n) | 57.5 (345) | 1.4 (59) | <0.001 |
| Previous PAF diagnosis, % (n) | 5.0 (30) | 2.4 (102) | <0.001 |
| Symptoms during exam, % (n) | |||
| Palpitations | 3.8 (23) | 9.1 (385) | <0.001 |
| Fatigue | 4.5 (27) | 4.8 (205) | 0.721 |
| Dyspnea | 1.0 (6) | 3.2 (136) | 0.003 |
| Dizziness | 4.0 (24) | 6.2 (264) | 0.031 |
| Syncope | 0.3 (2) | 0.2 (7) | 0.370 |
| Mental confusion | 0.0 (0) | 0.0 (1) | 0.707 |
| HF symptoms | 0.8 (5) | 0.9 (37) | 0.923 |
| Arrhythmia | 1.3 (8) | 3.2 (137) | 0.011 |
| Chest pain | 2.8 (17) | 7.8 (332) | <0.001 |
| No symptoms | 84.8 (509) | 74.7 (3170) | <0.001 |
| Relation between Holter findings and symptoms | 8.3 (50) | 6.7 (284) | 0.138 |
AF: atrial fibrillation; BMI: body mass index; COPD: chronic obstructive pulmonary disease; CVD: cardiovascular disease; ECG: electrocardiographic; HF: heart failure; MI: myocardial infarction; PAF: paroxysmal atrial fibrillation; PVCs: premature ventricular contractions; SD: standard deviation; WC: waist circumference.
Comparison between patients with AF, PAF or AFL and those in sinus rhythm during the monitoring period shows a significantly higher prevalence of the former among male patients (p<0.001) and older individuals (particularly in the 70-79 and >80 age-groups) (p<0.001). The proportions of patients with hypertension (76.3%) and with COPD (p<0.001) were also higher in patients with AF, PAF or AFL; there was a smaller, but still significant, excess of patients with dyslipidemia in this group. The prevalences of diabetes and hyperthyroidism were similar in the two groups.
The group with AF, PAF or AFL presented a significantly higher prevalence of previous stroke (56 patients, 9.3%; p=0.001) and MI (5.3%; p<0.001). They also had greater waist circumference (p=0.001), took less exercise (p=0.001) and consumed more alcohol (p=0.005). However, they also included more individuals who had never smoked (77.1% vs. 74.5% of those without these arrhythmias), more former smokers (19.2% vs. 17.6%) and fewer smokers (3.7% vs. 7.9%).
Regarding the reasons for referral for Holter study, patients with AF, PAF or AFL were significantly more likely to have been referred for palpitations (p=0.001), dizziness (p=0.001), weakness or exercise intolerance (p<0.001), chest pain (p=0.001) or syncope (p<0.005). Fatigue, dyspnea, mental confusion, HF, stroke and arrhythmia were equally frequent reasons in both groups.
There was also a significantly higher prevalence of AF, PAF or AFL in patients receiving medication (p=0.001) and in those with a previous diagnosis of any form of AF (p=0.001) or of PAF (p=0.001).
Most patients in both groups did not report symptoms during the Holter study, but the proportion who did not was significantly higher in the group with AF, PAF or AFL than in those without (84.8% vs. 74.7%, respectively; p=0.001). Palpitations and chest pain were more frequent in the latter group (p=0.001). The relation between Holter findings and symptoms was weak and the difference between the groups was not significant (8.3 vs. 6.7%, respectively; p=0.138).
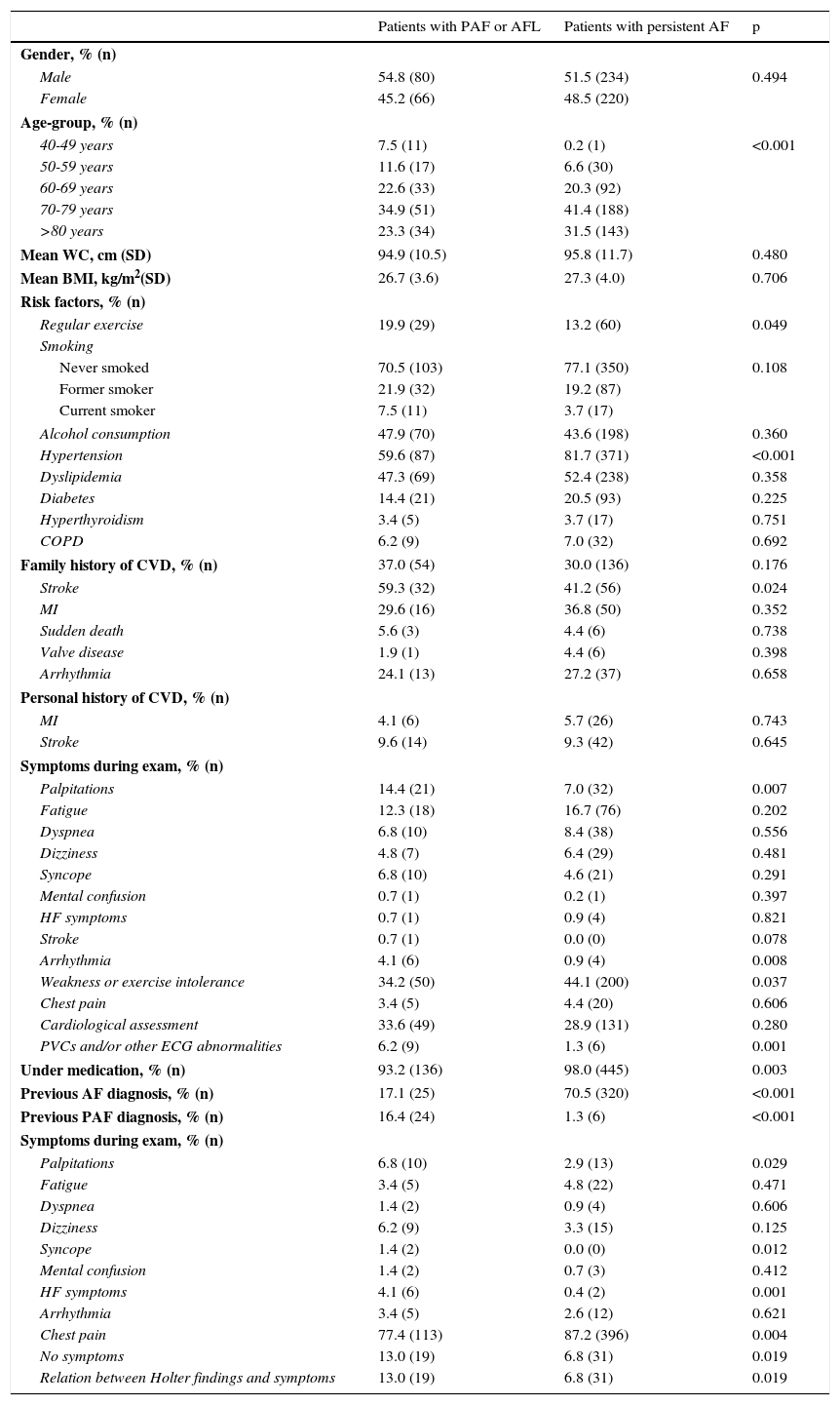
Characteristics of individuals with paroxysmal atrial fibrillation or atrial flutter compared to those with persistent atrial fibrillationSignificant differences were found between patients with PAF or paroxysmal typical AFL and those with persistent AF. PAF/AFL was more prevalent in younger patients (40-49, 50-59 and 60-69 age-groups) and less prevalent in the 70-79 and >80 age-groups (p<0.001), while more patients in the PAF/AFL group had a history of stroke (p<0.024) and fewer had hypertension (p<0.001) (Table 4).
Characteristics of individuals with paroxysmal atrial fibrillation or typical atrial flutter compared to those with persistent atrial fibrillation.
| Patients with PAF or AFL | Patients with persistent AF | p | |
|---|---|---|---|
| Gender, % (n) | |||
| Male | 54.8 (80) | 51.5 (234) | 0.494 |
| Female | 45.2 (66) | 48.5 (220) | |
| Age-group, % (n) | |||
| 40-49 years | 7.5 (11) | 0.2 (1) | <0.001 |
| 50-59 years | 11.6 (17) | 6.6 (30) | |
| 60-69 years | 22.6 (33) | 20.3 (92) | |
| 70-79 years | 34.9 (51) | 41.4 (188) | |
| >80 years | 23.3 (34) | 31.5 (143) | |
| Mean WC, cm (SD) | 94.9 (10.5) | 95.8 (11.7) | 0.480 |
| Mean BMI, kg/m2(SD) | 26.7 (3.6) | 27.3 (4.0) | 0.706 |
| Risk factors, % (n) | |||
| Regular exercise | 19.9 (29) | 13.2 (60) | 0.049 |
| Smoking | |||
| Never smoked | 70.5 (103) | 77.1 (350) | 0.108 |
| Former smoker | 21.9 (32) | 19.2 (87) | |
| Current smoker | 7.5 (11) | 3.7 (17) | |
| Alcohol consumption | 47.9 (70) | 43.6 (198) | 0.360 |
| Hypertension | 59.6 (87) | 81.7 (371) | <0.001 |
| Dyslipidemia | 47.3 (69) | 52.4 (238) | 0.358 |
| Diabetes | 14.4 (21) | 20.5 (93) | 0.225 |
| Hyperthyroidism | 3.4 (5) | 3.7 (17) | 0.751 |
| COPD | 6.2 (9) | 7.0 (32) | 0.692 |
| Family history of CVD, % (n) | 37.0 (54) | 30.0 (136) | 0.176 |
| Stroke | 59.3 (32) | 41.2 (56) | 0.024 |
| MI | 29.6 (16) | 36.8 (50) | 0.352 |
| Sudden death | 5.6 (3) | 4.4 (6) | 0.738 |
| Valve disease | 1.9 (1) | 4.4 (6) | 0.398 |
| Arrhythmia | 24.1 (13) | 27.2 (37) | 0.658 |
| Personal history of CVD, % (n) | |||
| MI | 4.1 (6) | 5.7 (26) | 0.743 |
| Stroke | 9.6 (14) | 9.3 (42) | 0.645 |
| Symptoms during exam, % (n) | |||
| Palpitations | 14.4 (21) | 7.0 (32) | 0.007 |
| Fatigue | 12.3 (18) | 16.7 (76) | 0.202 |
| Dyspnea | 6.8 (10) | 8.4 (38) | 0.556 |
| Dizziness | 4.8 (7) | 6.4 (29) | 0.481 |
| Syncope | 6.8 (10) | 4.6 (21) | 0.291 |
| Mental confusion | 0.7 (1) | 0.2 (1) | 0.397 |
| HF symptoms | 0.7 (1) | 0.9 (4) | 0.821 |
| Stroke | 0.7 (1) | 0.0 (0) | 0.078 |
| Arrhythmia | 4.1 (6) | 0.9 (4) | 0.008 |
| Weakness or exercise intolerance | 34.2 (50) | 44.1 (200) | 0.037 |
| Chest pain | 3.4 (5) | 4.4 (20) | 0.606 |
| Cardiological assessment | 33.6 (49) | 28.9 (131) | 0.280 |
| PVCs and/or other ECG abnormalities | 6.2 (9) | 1.3 (6) | 0.001 |
| Under medication, % (n) | 93.2 (136) | 98.0 (445) | 0.003 |
| Previous AF diagnosis, % (n) | 17.1 (25) | 70.5 (320) | <0.001 |
| Previous PAF diagnosis, % (n) | 16.4 (24) | 1.3 (6) | <0.001 |
| Symptoms during exam, % (n) | |||
| Palpitations | 6.8 (10) | 2.9 (13) | 0.029 |
| Fatigue | 3.4 (5) | 4.8 (22) | 0.471 |
| Dyspnea | 1.4 (2) | 0.9 (4) | 0.606 |
| Dizziness | 6.2 (9) | 3.3 (15) | 0.125 |
| Syncope | 1.4 (2) | 0.0 (0) | 0.012 |
| Mental confusion | 1.4 (2) | 0.7 (3) | 0.412 |
| HF symptoms | 4.1 (6) | 0.4 (2) | 0.001 |
| Arrhythmia | 3.4 (5) | 2.6 (12) | 0.621 |
| Chest pain | 77.4 (113) | 87.2 (396) | 0.004 |
| No symptoms | 13.0 (19) | 6.8 (31) | 0.019 |
| Relation between Holter findings and symptoms | 13.0 (19) | 6.8 (31) | 0.019 |
AF: atrial fibrillation; BMI: body mass index; COPD: chronic obstructive pulmonary disease; CVD: cardiovascular disease; ECG: electrocardiographic; HF: heart failure; MI: myocardial infarction; PAF: paroxysmal atrial fibrillation; PVCs: premature ventricular contractions; SD: standard deviation; WC: waist circumference.
A significantly higher proportion of patients took regular exercise in the PAF/AFL group (p=0.049), and compared to individuals with persistent AF, those with PAF/AFL had a significantly higher prevalence of palpitations (p=0.007), arrhythmia (p=0.008) and PVCs and/or other ECG abnormalities (p=0.001) and a significantly lower prevalence of weakness or exercise intolerance (p=0.037) and of medication (p=0.003).
With regard to symptoms during the exam, palpitations (p=0.029), syncope (p=0.012), arrhythmia (p=0.001), and a relation between Holter findings and symptoms were found significantly more often in the group with PAF/AFL than in the group with persistent AF. Conversely, absence of symptoms was more common in patients with persistent AF than in those with PAF/AFL (p=0.004).
Oral anticoagulationOf patients in sinus rhythm, 103 (2.4%) were taking oral anticoagulants for any reason; however, only 135 (29.9%) of those with persistent AF, 14 (12.8%) of those with PAF and six (26.1%) of those with typical AFL were anticoagulated.
DiscussionThis prospective study is probably the only one ever undertaken using 24-hour 12-lead ECG monitoring for the stated objectives.
Especial care was taken in collecting and interpreting the data, given that the referring GP was not aware that the exam had taken place or where.
The readings were interpreted and recorded in a specially designed dedicated database. Two of the arrhythmologists were blinded to the patient's identity and analyzed the readings independently; the findings were confirmed by a third team member who made the final decision in the event of disagreement.
The data obtained from the questionnaire were those usually collected during patient recruitment.
The overall prevalence of AF and AFL found in this study was even higher than expected (12.4%), which again highlights the importance of the link with stroke and the need for early diagnosis and prevention of thromboembolic events, including referral for invasive treatment such as radiofrequency catheter ablation or cryoballoon ablation.
Although 24-hour ECG monitoring is a well-known technique used routinely throughout the medical community, its usefulness for the detection of paroxysmal AF and AFL, which was the primary objective of this study, is frequently underestimated.
The high figure obtained for the prevalence of AF and AFL may have been affected by bias, the most important source of which is referral by GPs, who will have requested the exam according to their own clinical criteria, which were thus not predefined, although they were recorded for the purposes of the study. As noted above, the referring GPs were not aware of this study, and could not alter their clinical practice.
The prevalence found in this study is clearly different from those of Portuguese studies by Ascenção et al.8 (only 0.5%) and Gomes et al.9 (1.29%), who studied all primary health care users aged over 30 in part of the Greater Porto area. Both studies were based on retrospective analysis of medical records.
The prevalence of PAF in our study, as defined in the Introduction was 2.5%, a similar figure to the overall AF prevalence in the FAMA study. However, we believe that this prevalence is underestimated. If the proportion of patients with paroxysmal AFL is added, the overall prevalence is even higher.
As in the FAMA study, we decided to analyze patients with AF and typical AFL as a single group, since the latter is after all a type of arrhythmia, and one that frequently alternates with AF and carries a similar stroke risk. Although its standard treatment – cavotricuspid isthmus ablation – is different, it is often linked with the development of AF.
The FAMA study was prompted by the lack of data on the Portuguese population and variability in estimates of AF prevalence in European studies. It was a cross-sectional community study that analyzed a representative sample of the Portuguese population aged 40 and over, stratified by gender, age and geographical area, based on a study protocol that included a questionnaire and an ECG applied to a large sample (over 10000 randomly selected individuals from all regions of the country).
The main merit of the FAMA study was the fact that it assessed AF at a particular moment, when the ECG was taken. Its limitations were that the reading was very short (only a few seconds) and many study subjects refused to complete the questionnaire or undergo ECG testing. A total of 10447 subjects were assessed, but the number who fulfilled the inclusion criteria but refused to participate was much higher (15507). The reasons for refusal were not specified, but they may have been due to methodological considerations that are beyond the scope of this study.
In the present study, the participants had a clear reason to undergo 24-hour ECG monitoring, and it was not difficult to obtain their informed consent for an exam that would have been performed anyway.
The long duration of monitoring considerably increases the likelihood of recording an episode of AF, and so a higher prevalence would be expected. While even longer monitoring periods would further increase the chances of diagnosing AF, this is less practical, due to the effect on patient compliance, and is therefore limited to specific populations.10,11
Study participants who remained in sinus rhythm during the exam were asked if they had previously been diagnosed with AF or PAF, and 59 (1.4%) and 102 (2.4%), respectively, responded in the affirmative. Assuming that these responses were correct and ignoring the obvious possibility of overlap in responses from the same patient, it can be speculated that a further 3.8% should be added to the 12.4% prevalence calculated in our prospective study. This also means that the longer the monitoring period, the higher the prevalence of AF will be. This was demonstrated by Gladstone et al.,10 who studied the relation between AF and cryptogenic stroke in patients aged 55 years or older and recent stroke or transient ischemic attack. ECG monitoring over 30 days was superior to 24-hour monitoring, improving both diagnosis of AF more than five-fold and resulting therapeutic decisions, nearly doubling the rate of anticoagulation treatment at 90-day follow-up. There are, however, problems with prolonged monitoring, including patient compliance and artefacts.
Our study unequivocally demonstrates the value of 24-hour Holter monitoring for the diagnosis of PAF, since only 5.0% of the group diagnosed with PAF reported a previous diagnosis. By contrast, 57.5% of those with persistent AF on 24-hour monitoring had a previous diagnosis of persistent or permanent AF as defined in the international guidelines. This implies that for the latter patients, Holter study would have been requested as part of a rate control strategy as popularized following the results of the AFFIRM trial,12 but it also means that PAF was first diagnosed on the basis of Holter monitoring in 95% of cases, which has significant implications for clinical management of these patients.
The age distribution of individuals with paroxysmal AF or AFL was different from those with persistent AF, the former being significantly more frequent in younger age-groups (7.5% vs. 0.2% in those aged 40-49 and 11.6% vs. 6.6% in those aged 50-59). However, at older ages this pattern reversed, although the absolute numbers of patients diagnosed with PAF remained high and were never significantly lower than those with persistent AF. This means that PAF affects all ages and is not only a problem of aging.
It should be noted that 12-lead Holter monitoring is able to diagnose typical AFL according to the generally accepted definition, which may explain the relatively high prevalence (0.8%) of isolated typical AFL found in our study.
While the thromboembolic risk associated with AFL is similar to that of AF, treatment differs, since catheter ablation of AFL is more often curative than AF ablation, and pharmacological heart rate control with a lasting return to sinus rhythm is notoriously difficult to achieve in these patients.
AFL can coexist with or precede AF, and the relationship between them is complex. Some authors argue that in patients with coexisting AF and AFL, or even those with isolated AFL, catheter ablation of AF should be performed, with the possibility of associating it with cavotricuspid isthmus ablation of AFL.15
The high incidence of stroke found by Correia et al.3 in a geographically similar area to ours may well be linked to the high prevalence of AF found in the present study, in which significantly more patients with PAF/AFL had a history of stroke (p=0.001), with a prevalence of 9.3% in those with any kind of AF or AFL, and even more in those with PAF (p<0.024).
Comparison between patients with PAF/AFL and those with persistent AF shows a stronger association with hypertension in the latter group, although hypertension was significantly more prevalent in both groups than in those in sinus rhythm during the exam. This may mean that hypertension, considered a classic risk factor for AF, is less important in PAF, an early stage of the disease, the onset of which is due to triggering factors that are primarily electrical and centered around the pulmonary veins.13 This is particularly important given that the disease does not behave in the same way in all PAF patients: patients may have long periods without PAF punctuated by occasional symptomatic episodes, which could be due to a weaker trigger in a highly vulnerable atrial substrate, or – as in the individuals identified in our study – to strong and persistent triggers in an atrial substrate that is still able to resist sustainability of the arrhythmia. Bearing in mind that these are younger patients, since PAF is found at all ages, early invasive intervention (pulmonary vein isolation being demonstrably more effective than drug therapy), would appear to be the treatment of choice,10 especially as it is more likely to be successful when patients are referred earlier.14
Finally, as in other studies,4,9 the rates of oral anticoagulation were low: only 29.9% in patients with persistent AF and 12.8% in those with PAF. The explanation for the latter figure is simple: they had not been diagnosed.
ConclusionsThe prevalence of PAF found in a population who underwent continuous 24-hour electrocardiographic monitoring for diverse reasons was 2.5% and the overall AF prevalence was 12.4%, five times higher than in the FAMA study. The prevalence of PAF – albeit an underestimation – was 2.5% and its age distribution was more uniform; as such it is more prevalent in younger patients and less associated with risk factors such as hypertension, although with significantly higher rates of stroke. These patients are at an early stage of the disease and may be candidates for catheter ablation, which is frequently curative when applied at this stage.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors must have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence must be in possession of this document.
Funding sourcesThere was no external funding for the preparation of this article.
Conflicts of interestThis study was promoted by Forpoint – Instituto de Formação e Inovação na Saúde, received editorial assistance from Keypoint – Consultoria Científica, and received an unconditional grant from Sanofi Portugal.
The authors have no other conflicts of interest to declare.
We are grateful to all those who contributed directly or indirectly to this study:
Cardiac technicians: André Dias, Joana Dinis, Tatiana Pereira, Sara Costa, José Moutinho, Tânia Reis, Catarina Rua, Natália Costa, Diana Marques, Sandra Dias, Débora Daniel, Bárbara Ramos, Filipe Ascenso, Cristiana Varejão, Diana Ramos, Ana Teixeira, Ivo Marcos, and Pedro Silva.
Keypoint staff: Pedro Rocha, Lenia Nogueira, and João Martins.
Please cite this article as: Primo J, Gonçalves H, Macedo A, Russo P, Monteiro T, Guimarães J, et al. Prevalência da fibrilhação auricular paroxística numa população avaliada por monitorização contínua de 24 horas. Rev Port Cardiol. 2017;36:535–546.
