



A 44-year-old man with poorly differentiated lung adenocarcinoma (stage IV, T4N0M1a) was referred for a transthoracic echocardiogram (TTE) to assess for cardiac metastasis. Although there were no signs of left atrial invasion in parasternal and apical views, subcostal view on the TTE showed an image suggestive of a cardiac mass, with protrusion to the left atrium (LA) through the right inferior pulmonary vein (RIPV) (Figure 1A and Video 1). There were no other abnormal findings on the TTE. To clarify the extension of the cardiac mass, a transesophageal echocardiogram (TEE) was performed, revealing an exuberant tumoral mass in the RIPV, measuring 8.2 cm, with protrusion of 2.8 cm into the LA (Figure 1B and Video 2). Despite an apparent surgical cleavage plane in the LA, the cardiac mass showed complete invasion of the RIPV wall (Figure 1B). There were no masses adjacent to the left pulmonary veins. A chest computed tomography (CT) scan confirmed tumor invasion through the RIPV (Figure 1C and D). The patient then underwent successful surgical tumorectomy of the lung and RIPV mass and atrioplasty. The postoperative course was uneventful.
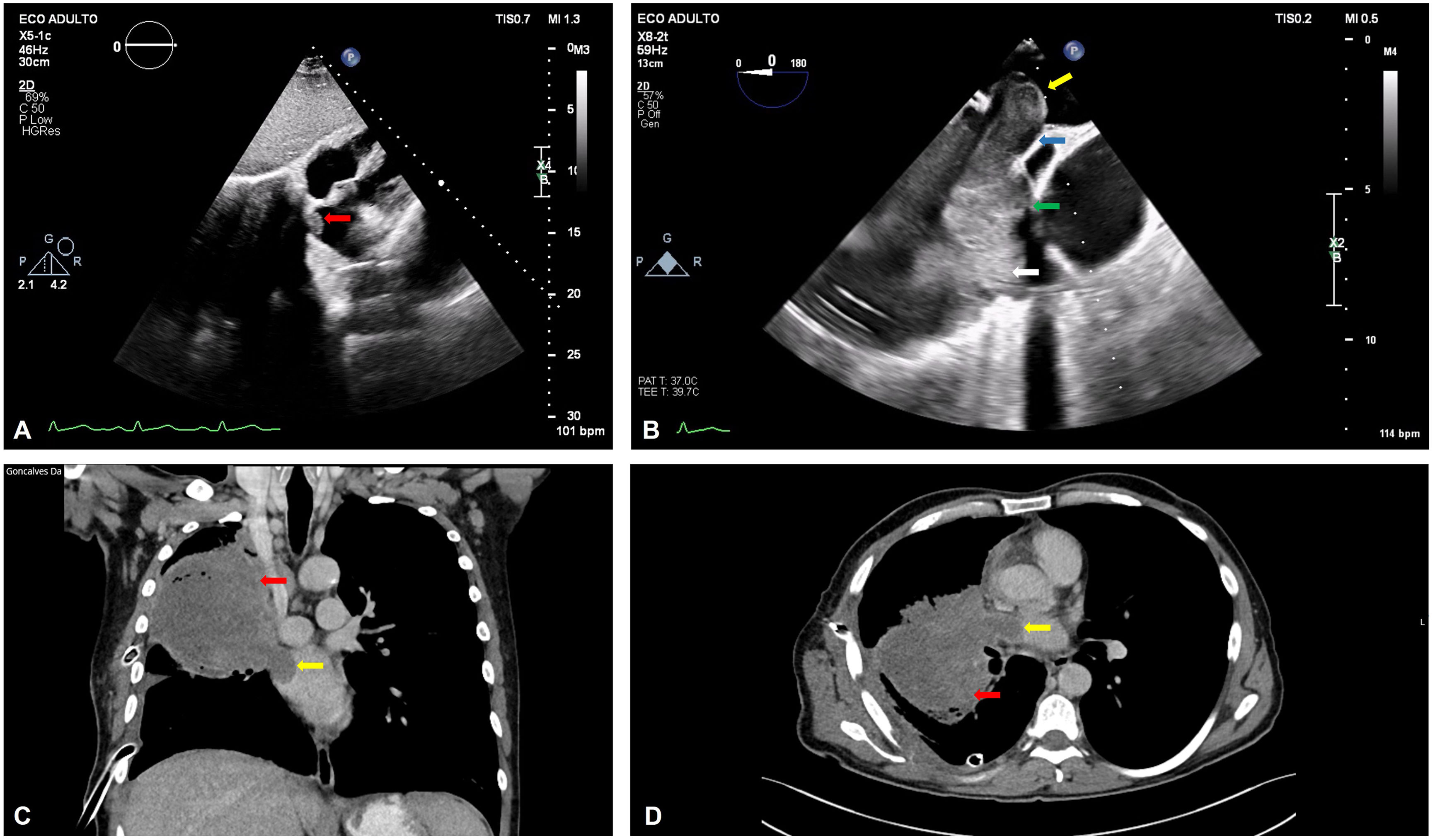
(A) Transthoracic echocardiogram (TTE) with an image suggestive of a cardiac mass with protrusion to the left atrium (LA) (red arrow); (B) TEE with an exuberant tumoral mass in the right inferior pulmonary vein (RIPV) with protrusion of 2.8 cm into the LA (yellow arrow); apparent surgical cleavage plane in the LA (blue arrow); area without surgical cleavage plane (green arrow); lung carcinoma (white arrow); (C) (coronal plane) and (D) (axial plane): chest computed tomography scan showing lung carcinoma (red arrow) invading the LA (yellow arrow).
Cardiac metastasis from lung carcinomas is rare.1 TTE is a crucial initial imaging modality as it can detect cardiac invasion to the pericardium or through the pulmonary veins.2,3 However, a high level of suspicion is needed, as a thorough scan may uncover minor findings that should prompt further imaging. CT, cardiac magnetic resonance imaging and positron emission tomography can provide further information on differential diagnosis of the mass.2–4
Conflicts of interestThe authors have no conflicts of interest to declare.
