



A 73-year-old male patient presented to the emergency department with a chief complaint of central chest pain for the previous three days. His medical history revealed heavy smoking, hypertension and atrial fibrillation (AF). His physical examination, ECG, chest radiograph and laboratory tests were unremarkable (AF at 70-80 bpm). Due to lack of response to conservative drug treatment, an aortic computed tomography angiography (CTA) scan was performed, which detected a bulge with a ‘mushroom cap’ appearance in the posterior wall of an aberrant right subclavian artery (ARSA), reported as limited dissection (Figure 1 and Supplementary Videos A and B). After multidisciplinary committee assessment, it was decided to perform endovascular repair. A Gore endoprosthesis in a nitinol-covered stent was anchored at the origin of the left subclavian artery and an Amplatzer Vascular Plug was used to exclude the dissection of the ARSA from circulation. Initially, the patient evolved favorably but a few days later he presented an acute recurrence of chest pain. A new CTA showed signs of type III endoleak (Supplementary Video C), and emergent endovascular repair was planned. Unfortunately, after anesthetic induction, the patient presented severe hypotension with hemodynamic instability that quickly evolved to cardiogenic shock, multiorgan failure and, eventually, death.
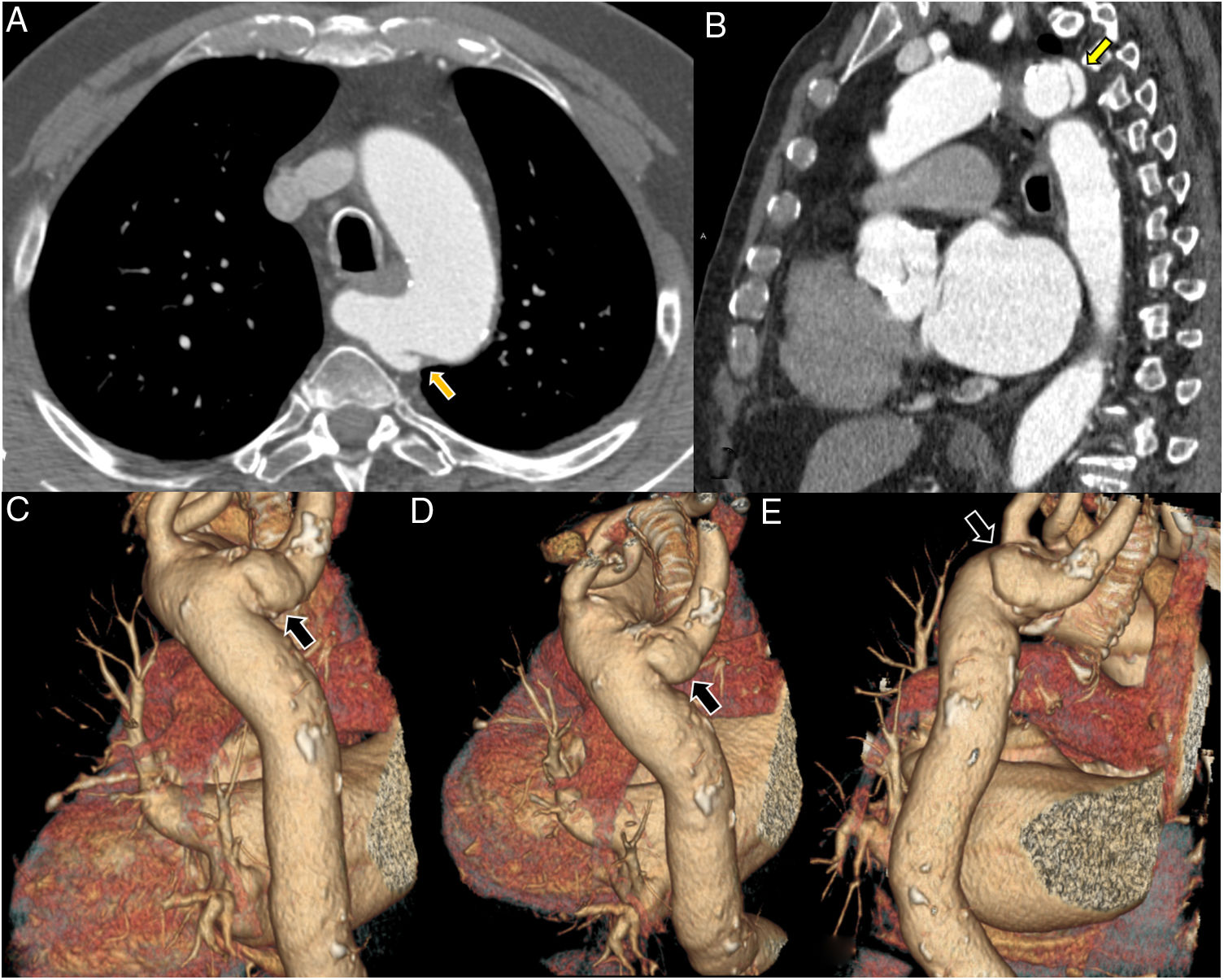
Computed tomography angiography of the aorta, axial view (A), multiplanar reformatting in sagittal view (B), and volume rendering in oblique posterior views (C-E). Focal bulging of 21 mm×8 mm with a ‘mushroom cap’ appearance at a Kommerell diverticulum of the aberrant right subclavian artery (yellow arrows in A and B, black arrows in C-E). The latter compresses the esophagus posteriorly along its course to the right and passes 8 mm posterior to the right posterolateral margin of the trachea. The aortic size is within normal range and no other structural abnormalities of the aorta are observed. Note that vascular repair at this location may entail technical difficulties, particularly anchoring the endoprosthesis at the origin of the right subclavian artery. In addition, total exclusion of the dissected segment cannot always be achieved.
Limited or subtle dissection is an uncommon form of acute aortic syndrome (AAS), and only a few case series have been published in the literature. Echocardiography and particularly CTA with cardiac gating can be considered the imaging modalities of choice because of their availability, speed and precision. The CTA appearance of limited dissection consists of an outward bulging oval or band-like luminal contour defect, resembling a mushroom cap. In the presence of these signs, emergent treatment is recommended, similarly to other types of AAS. Of note, Kommerell diverticulum has an increased risk of dissection and endovascular repair is a potential therapeutic strategy in limited dissections in this location, enabling the affected segment to be excluded. In this case, endovascular therapy was preferred over surgical treatment due to the patient's physical condition and the dissection type and location.
Conflicts of interestThe authors have no conflicts of interest to declare.
The following are the supplementary material to this article:
