







Rapid advances in cardiac magnetic resonance (CMR) and cardiac computed tomography angiography (CCTA) pose challenges for practicing physicians in terms of awareness of their indications, contraindications, advantages and pitfalls.
MethodsWe conducted a nationwide online survey assessing the familiarity, perceptions and patterns of use concerning these imaging modalities based on a questionnaire sent to all physician members of the Portuguese Society of Cardiology.
ResultsThe responses from 205 physicians (21% response rate) were analyzed. Roughly half of them requested less than one CMR (51%) or CCTA (52%) per week.
Suspected coronary artery disease in symptomatic patients with intermediate pretest probability was considered a good or excellent indication for CCTA by 59% of respondents when performed as a second-line exam, and by 29% as a first-line exam. Cardiac masses, congenital heart disease and cardiomyopathies were considered good or excellent indications for CMR by over 90% of respondents, while assessment of myocardial viability and acute myocardial infarction with normal coronary arteries were considered good or excellent indications by 75% and 65% of respondents, respectively. Less than half (39%) answered all the questions regarding contraindications for CMR correctly, and 15% were unaware that CMR does not involve ionizing radiation. The main reasons for not referring a patient for CMR were limited availability (45%) and cost (36%).
ConclusionsPortuguese cardiologists appear to be moderately aware of the indications, contraindications and advantages of these new imaging modalities. Greater efforts should be made to improve physician education on this subject in order to improve patient care.
A rápida evolução da ressonância magnética cardíaca (RMC) e da angio-TC cardíaca colocam desafios aos clínicos quanto ao conhecimento das suas indicações, contraindicações, vantagens e desvantagens.
MétodosEfetuámos um questionário online a todos os médicos sócios da Sociedade Portuguesa de Cardiologia com o intuito de avaliar a familiaridade, perceções e padrões de uso dos novos métodos de imagem.
ResultadosO questionário foi respondido por 205 médicos (21% do total). Cerca de metade disse requisitar menos de uma RMC (51%) ou angio-TC cardíaca (52%) por semana. A suspeita de doença coronária em doentes sintomáticos com probabilidade pré-teste intermédia foi considerada uma indicação boa ou excelente para angio-TC por 59% dos respondedores quando efetuada como exame de 2.a linha, e por 29% como exame de 1.a linha. Massas cardíacas, cardiopatias congénitas e miocardiopatias foram consideradas indicações boas/excelentes para RMC por mais de 90% dos respondedores, ao passo que a avaliação de viabilidade e enfarte com coronárias normais foram consideradas indicações boas/excelentes por 75 e 65% dos respondedores, respetivamente. Menos de metade (39%) respondeu corretamente a todas as perguntas acerca das contraindicações para RMC e 15% desconheciam que a RMC não utiliza radiação ionizante. As principais razões para não referenciar doentes para RMC foram a disponibilidade (45%) e o custo (36%).
ConclusõesOs cardiologistas portugueses parecem moderadamente familiarizados e conhecedores das indicações, contraindicações e vantagens dos novos métodos de imagem. Devem ser envidados esforços no sentido de melhorar estes indicadores por forma a permitir um uso racional destes exames complementares de diagnóstico.
As a result of recent technological advances, cardiac magnetic resonance (CMR) and cardiac computed tomography angiography (CCTA) are of increasing importance as diagnostic methods in clinical practice, and there has been a considerable broadening of indications for these exams.1–3 Nevertheless, the relative newness and rapid development of these imaging modalities pose challenges for practicing physicians in terms of awareness of their indications and contraindications, as well as their advantages and pitfalls compared to established methods.
The aim of this study was to assess the familiarity, perceptions and patterns of use concerning CMR and CCTA among Portuguese cardiologists.
MethodsPhysician members of the Portuguese Society of Cardiology (SPC) were invited to respond anonymously to an online questionnaire via a mailing in January 2011 to the email addresses contained in the SPC database. The study was identified as an initiative of the SPC's Working Group on Nuclear Cardiology, Magnetic Resonance and Cardiac Computed Tomography (GECNRMTC); the physicians were asked to respond without consulting any sources. A second mailing was sent in October 2011 to those who had not responded to the first; an electronic identification code was used in both mailings so that the same person could not respond more than once.
Questionnaires returned with demographic data only (n=18) were excluded from the analysis. To maintain the homogeneity of the population, responses from physicians in specialties other than cardiology, cardiothoracic surgery, pediatric cardiology or internal medicine were also excluded. This exclusion applied to four respondents: general and family medicine (n=2); physical medicine and rehabilitation (n=1); and radiology (n=1).
Results are presented as frequencies and percentages. Continuous variables are expressed as means ± standard deviation.
ResultsThe responses from 205 physicians (21% of SPC members contacted in the first mailing) were analyzed. The mean age of respondents was 47±11 years, most were male (67%, n=137) and had been specialists (89%, n=183) for 15±10 years. The great majority (87%, n=178) were cardiologists, and there were also 15 cardiac surgeons (7%), six pediatric cardiologists (3%), and six specialists in internal medicine (3%). The districts with the most respondents were Lisbon (38%, n=77), Porto (20%, n=40), Coimbra (9%, n=19) and Viseu (3%, n=7), although responses were received from all districts and autonomous regions of Portugal except Beja, Bragança and Guarda.
Most (80%, n=164) stated that they regularly performed transthoracic echocardiograms, 10% (n=20) CCTA, 7% (n=15) myocardial perfusion scintigraphy (MPS), and 7% (n=14) CMR; only 17% (n=34) stated they performed more than one of these imaging modalities, while another 17% (n=34) performed none of them. The vast majority (94%, n=192) said they were able to interpret transthoracic echocardiographic images, without an accompanying report, whereas only 17% (n=34) said they could make a correct diagnostic assessment of CMR images (Figure 1). The number of exams requested in a typical working week are shown in Figure 2. With regard to patterns of use, most respondents (60%, n=122) stated they had never requested a calcium score, 15% (n=30) CCTA, and 5% (n=11) CMR. In 18% (n=37) and 20% (n=40) of cases respectively, the last request for CCTA or CMR had been made more than six months previously.
?”. Cath: invasive coronary angiography; CCTA: cardiac computed tomography angiography; CMR: cardiac magnetic resonance; Echo: transthoracic echocardiography; SPECT: myocardial single-photon emission computed tomography.")
Responses to the question: “In which of the following imaging modalities do you think you would be capable of correctly interpreting the test based only on images or videos (without report)?”. Cath: invasive coronary angiography; CCTA: cardiac computed tomography angiography; CMR: cardiac magnetic resonance; Echo: transthoracic echocardiography; SPECT: myocardial single-photon emission computed tomography.
”. Stress echo: stress echocardiography; Ca score: calcium score. Other abbreviations as in Figure 1.")
Responses to the question: “How many of these imaging tests do you request in a typical working week? (If you work in more than one institution, please enter the total.)”. Stress echo: stress echocardiography; Ca score: calcium score. Other abbreviations as in Figure 1.
When asked to classify a set of eight indications for CMR, most respondents considered them good or excellent, except for coronary angiography (Figure 3). Cardiac masses, congenital heart disease and cardiomyopathies were considered good or excellent indications for CMR by over 90% of respondents, while assessment of myocardial viability and acute myocardial infarction with angiographically normal coronary arteries were considered good or excellent indications by 75% and 65%, respectively. The best indications for CCTA were considered to be assessment of asymptomatic patients with positive exercise ECG test, evaluation of aortocoronary bypasses, assessment of symptomatic patients with intermediate pretest probability of obstructive coronary artery disease (as second-line exam), and exclusion of coronary artery disease prior to valve surgery (Figure 4). Suspected coronary artery disease in symptomatic patients with intermediate pretest probability was considered a good or excellent indication for CCTA as the first-line exam by 29% of respondents.

Responses to the question: “How would you classify the following indications for cardiac magnetic resonance?”. AMI NCA: acute myocardial infarction with normal coronary arteries; ARVC: arrhythmogenic right ventricular cardiomyopathy; CHD: congenital heart disease; CMR: cardiac magnetic resonance; DK/NR: don’t know/no response; HCM: hypertrophic cardiomyopathy; MRA: magnetic resonance coronary angiography.
; B: symptomatic patient with intermediate pretest probability of obstructive coronary artery disease (as first-line test); C: asymptomatic patient with positive exercise ECG; D: asymptomatic patient with several cardiovascular risk factors; E: evaluation of aortocoronary bypasses; F: patient with known coronary artery disease; G: evaluation of coronary stents; H: exclusion of coronary artery disease prior to valve surgery”. DK/NR: don’t know/no response.")
Responses to the question: “How would you classify the following indications for cardiac computed tomography angiography?: A: symptomatic patient with intermediate pretest probability of obstructive coronary artery disease (as second-line test); B: symptomatic patient with intermediate pretest probability of obstructive coronary artery disease (as first-line test); C: asymptomatic patient with positive exercise ECG; D: asymptomatic patient with several cardiovascular risk factors; E: evaluation of aortocoronary bypasses; F: patient with known coronary artery disease; G: evaluation of coronary stents; H: exclusion of coronary artery disease prior to valve surgery”. DK/NR: don’t know/no response.
With regard to contraindications for CMR, the majority (91%) identified the presence of a pacemaker or implantable cardioverter-defibrillator, but a significant percentage considered that a mechanical valve or sternotomy wires also contraindicated the exam (45% and 25%, respectively) (Figure 5). Only 43% (79/185) responded correctly to all questions regarding contraindications for CMR.

Participants were then asked to classify in ascending order the mean radiation dose employed in the following four techniques: 99mTc MPS (stress-rest protocol), invasive diagnostic coronary angiography (without ventriculography), CCTA and CMR. Of the 173 physicians who answered this question, 40% (n=69) considered that MPS involved the highest mean radiation dose, while 27% (n=46) and 25% (n=44) chose CCTA and diagnostic coronary angiography, respectively. Around half of respondents (54%, n=94) believed that the mean radiation dose in CCTA is higher than in invasive coronary angiography, and 45% (n=78) believed it is higher in CCTA than in MPS. As for CMR, 15% (n=26) appear to be unaware that this technique does not involve ionizing radiation.
The participants were then asked to classify in ascending order the average cost of the following exams (without taking account of state funding or reimbursement): stress echocardiography, MPS, invasive diagnostic coronary angiography, CCTA and CMR. Of the 163 physicians who answered this question, 50% (n=81) considered invasive coronary angiography the most costly, while 40% (n=65) and 7% (n=12) chose CMR and MPS, respectively, and 2% (n=3) chose CCTA. Nevertheless, 66% (n=108) and 63% (n=102) believed CCTA to be more costly than MPS and invasive angiography, respectively. As for CMR, 67% (n=109) and 53% (n=87) believed that this technique is more costly than MPS and invasive angiography, respectively.
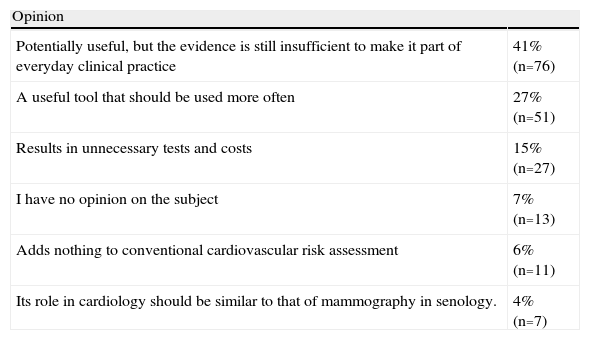
When asked about the main obstacle to wider use of CMR in clinical practice, 45% of respondents (n=84) cited problems of availability, 36% (n=66) cost, and 15% (n=27) lack of familiarity with the technique. The views of respondents with regard to calcium scoring are shown in Table 1.
Responses to the question: “Which of the following statements is closest to your opinion on coronary calcium score?”.
| Opinion | |
| Potentially useful, but the evidence is still insufficient to make it part of everyday clinical practice | 41% (n=76) |
| A useful tool that should be used more often | 27% (n=51) |
| Results in unnecessary tests and costs | 15% (n=27) |
| I have no opinion on the subject | 7% (n=13) |
| Adds nothing to conventional cardiovascular risk assessment | 6% (n=11) |
| Its role in cardiology should be similar to that of mammography in senology. | 4% (n=7) |
To our knowledge, this is the first study designed to assess the familiarity of Portuguese cardiologists with CMR and CCTA. In general, they appear to be moderately familiar with these imaging modalities and aware of their indications, contraindications, advantages and pitfalls. However, there appears to be some discrepancy between the acknowledged usefulness of these techniques and the extent to which they are used in clinical practice. For example, even though most respondents considered CMR a useful or very useful tool for a wide range of common clinical indications, a quarter had not requested CMR in the previous six months, and 5% had never requested it in their entire careers. This may mean that Portuguese cardiologists tend to reserve this exam for more complex cases in which conventional tests have been unable to provide an adequate clinical assessment, but hesitate to use CMR as an alternative to methods with which they are more familiar. Even in situations in which CMR has shown excellent performance, including assessment of myocardial viability,4 differential diagnosis of myocardial infarction with angiographically normal coronary arteries5 and in myocarditis,6 25–35% did not consider these sufficiently good reasons to refer patients for CMR. Perhaps less surprisingly, since the technique is relatively new and as yet not widely available in some regions, assessment of ischemia was considered an important indication for CMR by barely more than half of respondents. However, given that stress CMR has been shown to be superior to MPS and stress echocardiography in head-to-head comparisons,7,8 significant growth in use of this method is expected in the coming years.
Various reasons were given by participants in the study for not requesting CMR in clinical practice, limited availability being the one identified by the largest proportion (45%). Although the availability of the technique has increased considerably in recent years, particularly in large centers, where most of the respondents work, it is still not available in many public hospitals, which may be reluctant, or find it difficult, to refer patients to other institutions. At the same time, over a third of respondents cited the cost of CMR as the main limiting factor, a reason that appears to stem from the mistaken idea that CMR is more costly than, for example, MPS or invasive coronary angiography, when in fact it is less costly than either.9 As already pointed out, CMR is unavailable in many hospitals and is not covered by the national health service, which may be an obstacle to its wider use in clinical practice. On the other hand, only a minority of cardiologists (15%) cite unfamiliarity with the technique as a major reason for non-referral. However, a lack of familiarity is nonetheless evident, as reflected in the small proportion of respondents who consider themselves capable of correctly interpreting CMR images without an accompanying report, the percentage who are unaware of several of the contraindications for CMR, and the fact that 15% believe the technique involves ionizing radiation. These findings, which would have been worse if physicians experienced in the technique had been excluded from the analysis (data not presented), highlight the need for training in this area of cardiac imaging, which until recently received little attention in cardiology curricula.
Cardiologists appear to be slightly more familiar with CCTA than with CMR, with 29% of respondents considering themselves capable of interpreting the exams without an accompanying report; this may be a reflection of the greater availability of CCTA in Portugal and the fact that it is technically less complex. A significant proportion of cardiologists (almost 30%) consider the technique a good or excellent first-line exam to assess symptomatic patients with intermediate pretest probability of coronary artery disease, an innovation that is in line with recently published clinical guidelines.1,10 It thus appears that in general Portuguese cardiologists have an adequate understanding of the clinical usefulness of CCTA, identifying patients who would benefit most from the technique, namely those with intermediate or low pretest probability. Nevertheless, around a third of respondents had not requested CCTA in the previous six months, and 15% had never requested it in their careers. As with CMR, there appears to be a discrepancy between the acknowledged usefulness of the technique and the extent to which it is used in clinical practice, which may be due to problems of availability and/or to perceptions concerning cost, radiation dose, and others. With regard to cost, it is interesting that CCTA is seen by around two-thirds of respondents as being more costly than invasive coronary angiography or MPS, whereas in reality the average cost of CCTA is less than half that of either of these exams.9 The fact that a large proportion did not identify invasive diagnostic coronary angiography as the most costly exam of all those under analysis may be due to clinicians’ easy access to this technique and the fact that most such exams are performed within the national health service, and so referring physicians and patients are unaware of the costs involved. Regarding radiation dose, around half of respondents believe that the mean dose in CCTA is higher than in invasive coronary angiography or MPS. However, studies on everyday clinical practice have shown that this is not in fact the case, and mean radiation doses currently used in CCTA are significantly lower than in MPS, and similar to or lower than in diagnostic catheterization.11,12
The fact that invasive coronary angiography is more readily available than CCTA, together with misconceptions concerning their relative costs and radiation doses, may partly explain the high percentage of diagnostic catheterizations that reveal no obstructive coronary artery disease (41–62% in published series).13–15 Wider use of CCTA would help to minimize this problem, since the technique, when used appropriately, appears to reduce the number of normal coronary angiograms.16
With regard to coronary calcium score, it is interesting that, while only a small percentage of respondents consider that it provides no additional prognostic information to conventional cardiovascular risk assessment, most (60%) have never requested the test. It is probably underused, especially since it appears to be superior to other markers in terms of discriminatory power and risk reclassification17 and is a class IIa recommendation in European and American guidelines for cardiovascular risk stratification in asymptomatic individuals with intermediate risk.18,19 Portuguese cardiologists appear to recognize its potential, but feel the evidence is still insufficient to make it part of everyday clinical practice, which may reflect the lack of clear therapeutic guidelines based on calcium scores.
To summarize, there appears to be a certain lack of familiarity with CMR and CCTA on the part of Portuguese cardiologists. This is no doubt due in part to the relative newness of the two techniques and the fact that they are not readily available in cardiology departments. Their recent inclusion in cardiology intern training programs in Portugal may prove effective in improving knowledge and implementation of these methods. At the same time, there appears to be a need to strengthen continuing training in this area in Portugal.
Study limitationsCertain limitations of this study should be borne in mind. Firstly, only physicians with a valid email address in the SPC database were contacted and of these, only those who responded to the questionnaire were included in the analysis. This probably led to selection bias, resulting in over-representation of physicians with an interest and knowledge in this area, who would have been more likely to respond to a survey on the subject. Furthermore, since there has been no national or regional survey on the availability of CMR and CCTA, the relationship between availability and the responses obtained could not be analyzed. Even so, it seems clear that there are genuine problems with access which need to be addressed by the relevant bodies, as only in this way can appropriate diagnostic exams be selected for each clinical situation based on the evidence and cost/benefit ratios.
ConclusionsPortuguese cardiologists appear to be moderately aware of the indications, contraindications, advantages and pitfalls of CMR and CCTA. Patterns of use of these imaging modalities indicate that they are used less than would be expected from clinicians’ recognition of their usefulness, probably due to limited availability and certain misconceptions concerning the exams, particularly with regard to their costs and radiation dose. Greater efforts should be made to improve Portuguese cardiologists’ familiarity with CMR and CCTA, in order to achieve a more rational and appropriate use of these diagnostic techniques.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Ferreira AM, Bettencourt N, Matos P, et al. Familiaridade e perceções dos cardiologistas portugueses acerca da ressonância magnética cardíaca e angio-TC cardíaca - dimensão da tarefa à nossa frente. Rev Port Cardiol. 2013;32:601–608.
