
Recent studies have shown that the major risk factors for arterial thrombotic diseases are closely associated with venous thromboembolism (VTE). This study aimed to investigate the expression of CD3, CD4 and CD8 in T lymphocytes, the CD4/CD8 ratio and high-sensitivity C-reactive protein (hs-CRP) levels in patients with VTE, coronary artery atherosclerosis (CAA) and healthy subjects.
MethodsA total of 82 healthy subjects, 51 VTE patients and 114 CAA patients were recruited, and the expression of CD3, CD4 and CD8 in T lymphocytes and the CD4/CD8 ratio were determined. Serum hs-CRP was also measured.
ResultsCompared to healthy subjects, VTE patients had significantly reduced CD3 expression (p=0.019), comparable CD4 expression (p=0.868), significantly reduced CD8 expression (p<0.001) and increased CD4/CD8 ratio (p=0.044). However, VTE patients had comparable expression of CD3, CD4 and CD8 and CD4/CD8 ratio to CAA patients. In addition, among patients with VTE or CAA, the proportion of patients with reduced CD3+ and CD8+ T lymphocytes or increased CD4/CD8 ratio was significantly higher than in healthy subjects. In addition, hs-CRP in both VTE and CAA groups was significantly higher than in healthy subjects.
ConclusionsThe antigen recognition and signal transduction activation of T cells is significantly reduced in patients with VTE or CAA, and the killing effect of T cells on pathogens, including viruses, is also significantly compromised. In addition, inflammatory and immune mechanisms are involved in the occurrence and development of venous and arterial thrombosis.
Estudos recentes mostraram que os fatores de risco major das doenças trombóticas arteriais estão de forma muito próxima relacionados com a trombose venosa. Este estudo visou investigar as expressões CD3, CD4 e CD8 nos linfócitos T, a razão CD4/CD8 e a proteína reativa-C de alta sensibilidade (HsCRP) nos doentes com tromboembolismo venoso (TEV), com aterosclerose das artérias coronárias (AAC) e nos indivíduos saudáveis.
MétodosFoi recrutado um total de 82 indivíduos saudáveis, de 51 doentes com TEV e de 114 doentes com AAC e foram determinadas as expressões CD3, CD4 e CD8 nos linfócitos T e razão CD4/CD8. Foi também determinada a HsCRP sérica.
ResultadosQuando comparados com os indivíduos saudáveis, os doentes com TEV tiveram expressões significativamente reduzidas: CD3 (p=0,019) comparável com a expressão CD4 (p=0,868) e CD8 (p<0,001) e razão CD4/CD8 (p=0,044) aumentada. No entanto, os doentes com TEV tiveram expressões CD3, CD4 e CD8 e razão CD4/CD8 comparáveis aos doentes com AAC. Além disso, os resultados mostraram, nos doentes com TEV ou AAC, a proporção de doentes com expressão CD3+ reduzida e linfócitos CD8+T ou razão CD4+/CD8+ ou razão aumentada CD4+/CD8+ significativamente aumentada, quando comparados com os indivíduos saudáveis. Além disso, a HsCRP no grupo com TEV e no grupo com AAC foi significativamente superior do que no grupo dos indivíduos saudáveis.
ConclusãoO reconhecimento do antigénio e a ativação do sinal da transdução das células T estão significativamente reduzidos nos doentes com TEV ou com AAC e o efeito mortífero das células T nos patogéneos, incluindo os vírus, está significativamente comprometido. Além disso, os mecanismos inflamatórios e imunológicos estão envolvidos na ocorrência e no desenvolvimento da trombose venosa e arterial.
atherosclerosis
coronary artery atherosclerosis
confidence interval
high-density lipoprotein cholesterol
high-sensitivity C-reactive protein
low-density lipoprotein cholesterol
odds ratio
total cholesterol
triglycerides
venous thromboembolism
Previously, venous thromboembolism (VTE) was regarded as a separate disease from arterial thromboembolism.1 However, this hypothesis has been challenged. In 2003, Prandoni et al.2 reported that transient venous thrombosis patients had more atherosclerotic plaques in the carotid arteries, suggesting that atherosclerosis can cause venous thrombosis or that the two conditions share risk factors. In the Lancet in 2007, Srensen et al.3 assessed the hospitalization rate due to acute arterial cardiovascular events over 20 years in a cohort of venous thrombosis patients, and found that VTE patients had significantly increased risk for cardiovascular events. In 2008, a meta-analysis on the correlation between cardiovascular risk factors and VTE showed that the major risk factors for atherothrombotic disease were significantly associated with VTE.4 It has been suggested that cardiovascular risk factors are also directly involved in the pathogenesis of VTE. To further investigate the potential mechanisms underlying this correlation, it would be helpful to elucidate the pathogenesis of VTE and to screen high-risk subjects for primary and secondary prevention of VTE. On the basis of previous findings, this study was undertaken to compare T-cell immune function in VTE patients, CAA patients and healthy controls, to elucidate whether inflammatory immunity is involved in the occurrence and development of venous thrombosis as in atherosclerosis. We further investigated T-cell immune function, hs-CRP and cardiovascular risk factors in VTE patients, CAA patients and healthy controls, and also evaluated the correlation between VTE and arterial thrombosis, aiming to explore the pathogenesis and risk factors of VTE.
MethodsSubjectsA total of 51 inpatients with clinically proven VTE but without CAA were recruited from the Affiliated Tongji Hospital of Tongji University, Shanghai, between January 2008 and August 2012. In addition, 114 inpatients with CAA and 82 healthy subjects were also enrolled as controls. The diagnostic criteria for pulmonary embolism were any two of the following: (1) selective pulmonary angiography showing pulmonary artery occlusion or filling defect; (2) pulmonary ventilation-perfusion scan showing single or multiple perfusion defect, normal or abnormal ventilation, and ventilation-perfusion mismatch; (3) clinical diagnosis based on presence of risk factors for pulmonary embolism, other cardiopulmonary diseases being excluded by clinical presentations, electrocardiography and chest X-ray. Echocardiography, chest CT scan, arterial gas analysis, detection of D-dimers and Wells score supported the diagnosis of pulmonary embolism. For VTE patients and CAA patients, malignant tumors, autoimmune diseases, administration of immunosuppressants, and arterial thrombosis were excluded. Healthy controls who underwent physical examination were recruited from the outpatient clinic. The study was approved by the ethics committee of Tongji Hospital and written consent was obtained from each patient before participation in the study.
Sample collectionSamples were collected on admission or during hospital visits. Fasting blood (2 ml) was collected from the cubital vein into an ET tube containing dipotassium EDTA.
Preparation of samplesAnticoagulated blood (50 μl) was added to a tube and mixed with the corresponding antibody (10 μl; Beckman Coulter, USA) followed by incubation at room temperature in the dark for 20 min. After addition of hemolysin (250 μl), the preparation was incubated in the dark for 60 min, and following addition of normal saline (500 μl), was further incubated in the dark for 15 min and then centrifuged at 1500 rpm for 15 min. The supernatant was removed and the sediment collected and mixed in 300 μl of normal saline, followed by detection.
DetectionIOTest CD3 (Beckman Coulter, France), and CD4-FITC/CD8-PE (Beckman Coulter, France) monoclonal antibody test kits were used in this study. An EPICS XL-II flow cytometer (Beckman Coulter, USA) was employed for the detection of T-cell surface differentiation antigens. The prepared samples were subjected to flow cytometry, and the data were automatically recorded.
Biochemical analysisBiochemical analysis was performed during hospital stay or routine physical examination. Fasting venous blood was collected in the morning. A fraction of blood was subjected to detection of hs-CRP, fasting blood glucose, total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) with a Hitachi 7170 automated biochemical analyzer, and the remaining blood was used for the detection of T-cell differentiation antigens by flow cytometry (EPICS XL-II, Beckman Coulter, USA).
Statistical analysisThe statistical analysis was performed with SPSS version 14.0 for Windows. Continuous data with normal distribution were expressed as mean ± standard deviation. Comparisons between multiple groups were performed with one-way analysis of variance, and those between two groups with Fisher's LSD test. Continuous data with a non-normal distribution were expressed as median (interquartile range) and compared with the Wilcoxon test. Discrete data were expressed as frequency and percentage, and compared with the chi-square test. Odds ratios (OR) and 95% confidence intervals (CI) were calculated. A value of two-sided p<0.05 was considered statistically significant.
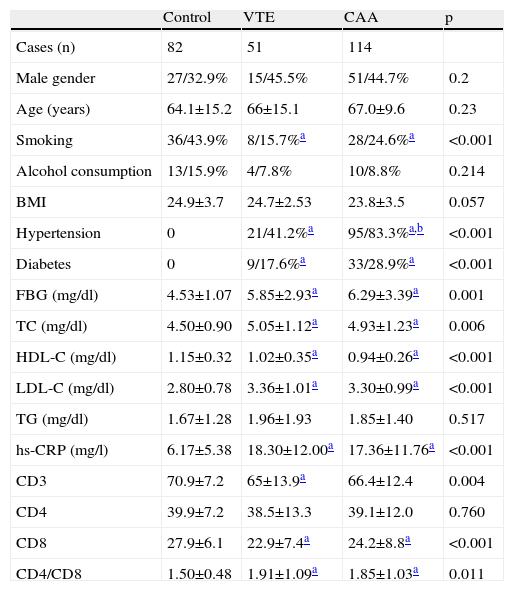
ResultsExpression of CD3, CD4 and CD8 and CD4/CD8 ratio in the three groups at baselineThe CD3, CD4, and CD8 levels and CD4/CD8 ratio are shown in Table 1. No significant differences were observed in age, gender, history of alcohol consumption or body mass index between the three groups (p>0.05). The proportion of CAA patients with hypertension was significantly higher than that of VTE patients (p>0.05). There was no significant difference in the proportion of diabetes patients between the VTE and CAA groups, and mean fasting blood glucose was similar between VTE and CAA, but significantly higher than in healthy subjects (p=0.001). TC and LDL-C in the VTE and CAA groups were significantly increased compared with healthy subjects. HDL-C in the VTE and CAA groups was lower than in healthy subjects, while TG levels were comparable between the three groups (p=0.517). In the VTE and CAA groups hs-CRP was significantly higher than in healthy subjects, but there was no significant difference between VTE and CAA (p=0.648).
Population characteristics and expression of CD3, CD4 and CD8 and CD4/CD8 ratio in the three groups at baseline.
| Control | VTE | CAA | p | |
| Cases (n) | 82 | 51 | 114 | |
| Male gender | 27/32.9% | 15/45.5% | 51/44.7% | 0.2 |
| Age (years) | 64.1±15.2 | 66±15.1 | 67.0±9.6 | 0.23 |
| Smoking | 36/43.9% | 8/15.7%a | 28/24.6%a | <0.001 |
| Alcohol consumption | 13/15.9% | 4/7.8% | 10/8.8% | 0.214 |
| BMI | 24.9±3.7 | 24.7±2.53 | 23.8±3.5 | 0.057 |
| Hypertension | 0 | 21/41.2%a | 95/83.3%a,b | <0.001 |
| Diabetes | 0 | 9/17.6%a | 33/28.9%a | <0.001 |
| FBG (mg/dl) | 4.53±1.07 | 5.85±2.93a | 6.29±3.39a | 0.001 |
| TC (mg/dl) | 4.50±0.90 | 5.05±1.12a | 4.93±1.23a | 0.006 |
| HDL-C (mg/dl) | 1.15±0.32 | 1.02±0.35a | 0.94±0.26a | <0.001 |
| LDL-C (mg/dl) | 2.80±0.78 | 3.36±1.01a | 3.30±0.99a | <0.001 |
| TG (mg/dl) | 1.67±1.28 | 1.96±1.93 | 1.85±1.40 | 0.517 |
| hs-CRP (mg/l) | 6.17±5.38 | 18.30±12.00a | 17.36±11.76a | <0.001 |
| CD3 | 70.9±7.2 | 65±13.9a | 66.4±12.4 | 0.004 |
| CD4 | 39.9±7.2 | 38.5±13.3 | 39.1±12.0 | 0.760 |
| CD8 | 27.9±6.1 | 22.9±7.4a | 24.2±8.8a | <0.001 |
| CD4/CD8 | 1.50±0.48 | 1.91±1.09a | 1.85±1.03a | 0.011 |
BMI: body mass index; FBG: fasting blood glucose; HDL-C: high-density lipoprotein cholesterol; hs-CRP: high-sensitivity C-reactive protein; LDL-C: low-density lipoprotein cholesterol; TC: total cholesterol; TG: triglycerides.
The T lymphocyte subsets were compared between the three groups. The number of CD3+ (p=0.019) and CD8+ T cells (<0.001) was significantly lower, and the CD4/CD8 ratio was markedly higher (p=0.044), but CD4+ T cells remained unchanged (p=0.868) in the VTE group compared with healthy subjects. In addition, compared with healthy subjects, the number of CD3+ (p=0.019) and CD8+ T cells (<0.001) reduced markedly, and the CD4/CD8 ratio (p=0.044) increased dramatically, but CD4+ T cells remained unchanged (p=0.868) in the CAA group. However, there were no significant differences in the number of CD3+, CD4+, CD8+ T cells or CD4/CD8 ratio between the VTE and CAA groups.
Compared with healthy controls, VTE patients had significantly lower CD3 expression (p=0.019), unchanged CD4 expression (p=0.868), significantly reduced CD8 expression (p<0.001) and dramatically increased CD4/CD8 ratio (p=0.044), while CAA patients had significantly reduced CD3 expression (p=0.019), unchanged CD4 expression (p=0.868), significantly reduced CD8 expression (p<0.001) and significantly increased CD4/CD8 ratio (p=0.044). However, there were no significant differences in the expression of CD3, CD4 and CD8 or CD4/CD8 ratio between CAA and VTE patients.
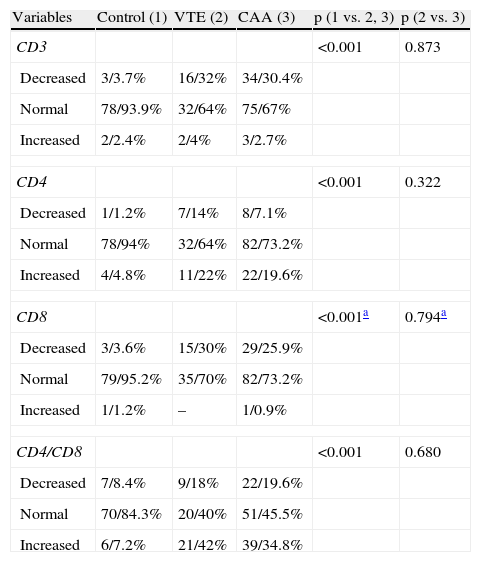
Comparisons of expression of CD3, CD4 and CD8 and CD4/CD8 ratioThe normal ranges were as follows: CD3: 60–85%; CD4: 24.5–48.8%; CD8: 18.5–42.1%; CD4/CD8: 1.02–1.94:1. The proportions of patients with reduced, normal and increased expression of CD3, CD4 and CD8 were calculated independently and compared with the chi-square test. This showed that these proportions were significantly different between VTE patients, CAA patients and healthy controls. The major differences were the high proportion of patients with reduced expression of CD3 and CD8, and the high proportion of patients with increased CD4/CD8 ratio (p<0.001). However, there was no significant difference between the CAA and VTE groups (p>0.05). In the VTE group, 18 patients had abnormal CD3 expression (decreased in 16 and increased in two), 18 had abnormal CD4 expression (reduced in seven and increased in 11), 15 had abnormal CD8 expression (reduced in all), and 30 had abnormal CD4/CD8 ratio (reduced in 9 and increased in 21). Moreover, about 42% of patients had increased CD4/CD8 ratio (Table 2). The proportion of patients with increased CD4/CD8 ratio in the VTE and CAA groups was higher than in healthy controls.
Expression of CD3, CD4 and CD8 and CD4/CD8 ratio in the three groups.
| Variables | Control (1) | VTE (2) | CAA (3) | p (1 vs. 2, 3) | p (2 vs. 3) |
| CD3 | <0.001 | 0.873 | |||
| Decreased | 3/3.7% | 16/32% | 34/30.4% | ||
| Normal | 78/93.9% | 32/64% | 75/67% | ||
| Increased | 2/2.4% | 2/4% | 3/2.7% | ||
| CD4 | <0.001 | 0.322 | |||
| Decreased | 1/1.2% | 7/14% | 8/7.1% | ||
| Normal | 78/94% | 32/64% | 82/73.2% | ||
| Increased | 4/4.8% | 11/22% | 22/19.6% | ||
| CD8 | <0.001a | 0.794a | |||
| Decreased | 3/3.6% | 15/30% | 29/25.9% | ||
| Normal | 79/95.2% | 35/70% | 82/73.2% | ||
| Increased | 1/1.2% | – | 1/0.9% | ||
| CD4/CD8 | <0.001 | 0.680 | |||
| Decreased | 7/8.4% | 9/18% | 22/19.6% | ||
| Normal | 70/84.3% | 20/40% | 51/45.5% | ||
| Increased | 6/7.2% | 21/42% | 39/34.8% | ||
VTE, including deep vein thrombosis and pulmonary embolism, has high morbidity, mortality and misdiagnosis rate.5 A US study reported the incidence of deep vein thrombosis as 0.5%.6 In the past 20 years, the incidence of pulmonary embolism has increased in Asia, including China, Japan, Thailand, Singapore and Taiwan.7 The pathogenesis and etiology of VTE are still unclear. Virchow's triad (hypercoagulability, hemodynamic changes [stasis, turbulence] and endothelial injury/dysfunction) is still used to explain the pathogenesis of VTE.8 However, this concept does not always explain the occurrence of acquired VTE in clinical practice. In the American College of Chest Physicians guidelines for antithrombotic therapy and prevention of thrombosis, patients receiving surgery are stratified according to risk factors, and anti-coagulation therapy for prevention of VTE is based on these guidelines. However, the incidence of VTE continues to increase.
The pathogenesis of atherosclerosis (AS) has been investigated for more than 150 years. Currently, AS is regarded as a chronic inflammatory disease. Statins may delay the occurrence and development of AS through their anti-inflammatory activity, making them a milestone in the treatment of AS. Until recently, venous thrombosis was regarded as a separate disease from AS, but there is correlation between the two, and they share risk factors that include obesity, diabetes, hypertension, dyslipidemia (hypertriglyceridemia and low HDL-C) and smoking. Our results showed that the traditional risk factors for CAA (such as hypertension, hyperglycemia, TC, HDL-C and LDL-C) were significantly associated with venous thrombosis. The correlation between AS and VTE provides support for investigation of the pathogenesis of VTE, screening of high-risk populations and the development of strategies for primary and secondary prevention of VTE.
Since 2004, we have been engaged in basic and clinical investigation of VTE, employing microarray assay and fluorescence quantitative PCR to detect mRNA expression in peripheral blood of VTE patients. This showed that mRNA expression of T-lymphocyte proteins is significantly reduced, particularly CD3G, CD3D, CD247, ZAP-70 and T-cell granzyme A and B. This suggests that the cytotoxic activity of T cells is impaired.10 In AS, T lymphocytes are recruited and activated and inflammatory cytokines are secreted, which are observed in different stages in the occurrence and development of AS. Whether venous thrombosis is an inflammatory process like arterial thrombosis, and whether impaired T cell function is involved in the occurrence and development of VTE, are still largely unclear.
On the basis of our previous findings, VTE in patients and outpatients were recruited from Tongji Hospital between January 2008 and August 2012. Patients with CAA were also enrolled, as well as healthy subjects as controls. T-cell function and serum hs-CRP levels were determined in these subjects. Impaired T-cell function was observed in VTE patients, characterized by reduced expression of CD3 and CD8, increased CD4/CD8 ratio and unchanged CD4 expression. Reduction in CD3+ T cells suggests compromised antigen recognition and transduction activation, while reduction in CD8 indicates a decrease in CD8+ cytotoxic T lymphocytes, which are the major effector cells of cellular immunity. This suggests that direct killing of pathogens by T cells is compromised. The CD4/CD8 ratio is a sensitive indicator for clinically determining immune function, and when increased suggests that cellular immunity is compromised, with reduced activation and killing activity. However, CD4+ T cells, the cells principally responsible for assisting other leukocytes and regulating the immune response, were not affected. At the same time, our findings also revealed that the impaired T cell function in CAA patients was similar to that in VTE patients, and both presented with impaired T-cell immune function.
Activation, cloning and proliferation of T cells require the presence of specific antigens. Certain autoantibodies and pathogens (such as Chlamydia pneumoniae, herpes simplex and cytomegalovirus) serve as antigens to activate T lymphocytes. Infection is a major cause of AS, as has been reported in numerous studies.9 In 2006, Smeeth et al. reported that the occurrence of VTE was associated with infection, usually occurring within two weeks.11 In 2011, Schmidt et al. retrospectively investigated 15 009 cases of VTE and showed that risk for VTE was increased twofold in patients with infection, especially within two weeks of infection, gradually declining thereafter.12 In the present study, about 50% of VTE patients had concomitant infection, and an additional 16% of them developed VTE within two weeks after bone fracture. In 2010, we reported venous thrombi in multiple organs of a patient who died of SARS,13 and we have also found virus-like structures in the lymph nodes of a young patient with pulmonary hypertension.14 Whether the pathogens in these lesions cause pathological changes directly or by eliciting an immune response is still poorly understood. Other risk factors might also contribute to the pathogenesis of VTE.
Infection, especially viral infection, may attack T cells and induce damage to these cells, which can affect the immune system, leading to secondary immunodeficiency. However, cancer, severe malnutrition, medication with immunosuppressants and other factors (old age, obesity, diabetes, hypertension and smoking) are also accompanied by varying degrees of immune dysfunction. Thus, we speculate that immune mechanisms are involved in the occurrence and development of arterial and venous thrombosis.
Among inflammatory cytokines, hs-CRP is a potent marker for inflammation and can be used to predict risk for cardiovascular diseases; increased hs-CRP is closely linked to the severity of coronary lesions. In the present study, hs-CRP was significantly increased in both VTE and CAA patients, suggesting that inflammatory mechanisms are involved in the pathogenesis of venous thrombosis.
Taking these factors together, we speculate that inflammation and immune mechanisms are the bridge between AS and VTE, their shared risk factors leading to damage to vascular endothelial cells by inducing an inflammatory immune response and interfering with the coagulation balance, resulting in venous or arterial thrombosis. However, the methodology of this study is relatively simple, which is a limitation. In-depth clinical trials and studies in animal models are required to elucidate the symptoms and pathogenesis of VTE and their relation with the immune response. However, the inflammation and immunity theory of VTE inspires us and provides support for further studies on the pathogenesis of VTE.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
