



Atherosclerosis is a diffuse arterial disease, discontinuously distributed, that is not always linear in its pathophysiological significance. Starting with a paradigmatic clinical case, we review the hemodynamic techniques that are currently available for the assessment of this condition. We present the case of a male patient with known diffuse atherosclerotic disease, who had previously undergone angioplasty, in which angiography was repeated after acute pulmonary edema, with worsening left ventricular function and local ischemia documented by myocardial scintigraphy. The angiogram showed an intermediate lesion in the left anterior descending artery, not related to the ischemic territory. The significance of the lesion was evaluated anatomically with intravascular ultrasound, and functionally by determining fractional flow reserve with a pressure wire. We review the pathophysiology of the disease and the parameters used for overall evaluation, focusing on catheterization laboratory techniques and their indications and contribution to the diagnosis and treatment of coronary atherosclerosis.
A aterosclerose é uma doença arterial difusa, com distribuição descontínua, cujo significado fisiopatológico nem sempre é linear. A partir de um caso paradigmático faz-se a revisão das técnicas actualmente disponíveis na sala de hemodinâmica, para este fim. Trata-se de um paciente do sexo masculino, com aterosclerose coronária difusa conhecida, previamente submetido a intervenção percutânea, que realiza coronariografia após descompensação por edema agudo do pulmão, com deterioração da função ventricular esquerda e documentação de isquémia em cintigrafia de perfusão miocárdica. No cateterismo foi observada uma lesão de significado angiográfico intermédio na artéria descendente anterior, em território diferente do documentado por cintigrafia. Procedeu-se primeiro à avaliação do significado da lesão quer anatómico, através de ultrassonografia intravascular, quer funcional, através da determinação da reserva coronária com guia de pressão. Revemos a fisiopatologia desta doença, parâmetros da sua avaliação global, focando estas técnicas per-cateterismo, suas indicações e contribuição no diagnóstico e terapêutica da aterosclerose coronária.
The effect of atherosclerosis on vessels is discontinuous in both space and time, giving rise to acute and chronic clinical syndromes 1. Accurate assessment of its progression requires different diagnostic techniques, invasive and non-invasive, to guide the choice of the most effective treatment.
Case reportWe present the case of a 62-year-old male patient, hypertensive and dyslipidemic, a moderate smoker (1 pack/day), followed in the cardiology outpatient clinic for coronary disease, with CCS class I stable angina. In 2001 catheterization showed 2-vessel coronary disease affecting the first septal branch (99 % proximal lesion) and the right coronary artery (RCA), the mid third of which was occluded and perfused retrogradely (Rentrop grade 2) by collaterals from the left coronary artery. The latter lesion was treated by angioplasty with a 3 × 20mm balloon and a 3 × 23mm ACS Tetra stent was implanted, resulting in TIMI flow 3. One month later he was hospitalized for inferior ST-segment elevation myocardial infarction following acute occlusion of the stent in the RCA, which was dilated with a 3 × 20mm balloon, with re-establishment of TIMI flow 3. He remained asymptomatic for three years until 2004, when following recurrence of angina catheterization was repeated, and revealed in-stent occlusion of the RCA and a 75 % lesion in the proximal third of the circumflex artery, which was treated by implantation of a 3.5 × 13mm Cypher stent (with TIMI flow 3).
The patient was stable and asymptomatic until May 2009, when he was admitted to the emergency department with acute pulmonary edema. The transthoracic echocardiogram showed worsening parameters compared to the previous exam, with left ventricular dilatation, slightly impaired systolic function due to inferoposterior akinesia and hypokinesia of the septum, and mild mitral and aortic regurgitation. Myocardial perfusion scintigraphy showed an ischemic area in the septal wall and necrosis of the inferior wall; left ventricular ejection fraction was calculated at 49.9 %. The patient was asymptomatic under therapy with aspirin 100mg, simvastatin 40mg, furosemide 40mg, telmisartan 40mg, nitroglycerin 5mg SC, isradipine 5mg and alprazolam 0.5mg.
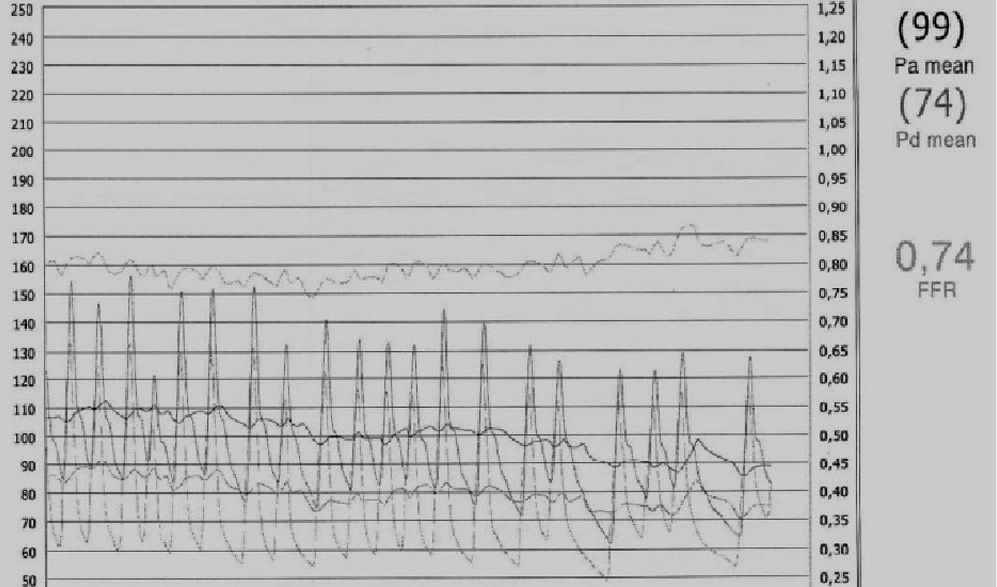
The patient was referred for selective coronary angiography (Figura 1), which showed a 50–75 % lesion in the mid third of the left anterior descending artery (LAD), patent stent and no de novo lesions in the circumflex, and in-stent occlusion of the RCA, with Rentrop grade 3 retrograde flow from the left-to-right collaterals. Since there appeared to be an intermediate lesion in the LAD, an important vessel both in itself and because of the collaterals supplying the RCA, and the ischemia appeared to be located only in the septal region, functional assessment was carried out with a pressure wire, using a Certus probe and a RADI Analyzer Xpress (St. Jude Medical). After maximal hyperemia with a 60-μ bolus of adenosine, fractional flow reserve (FFR) was measured as 0.74 (Figura 2). The lesion was then characterized by intravascular ultrasound (IVUS) using a Boston Scientific iLab system and an Atlantis SR Pro imaging catheter, revealing atheromatosis in the mid third of the vessel, with a minimum area of 2mm 2, a 30° calcium arc at 3 o'clock, and no significant involvement of the ostium of the first diagonal branch, an important vessel, proximal to the lesion (Figura 3). A 3 × 24mm Endeavor stent was accordingly implanted directly, released at 14atm and overdilated with a 3 × 15mm non-compliant (NC) balloon, after angiographic evaluation. IVUS (Figura 4) revealed inadequate stent expansion (maximum diameter 2.61mm), and so it was further dilated, this time with a 3.5 × 15mm NC balloon, resulting in a final diameter of 3.8mm by IVUS (9.1mm 2), and TIMI 3 flow.




The patient was discharged after 24 hours with no recorded complications. Six months after the procedure he is asymptomatic.
DiscussionThere are several stages in the development of atherosclerosis, the first of which is characterized by endothelial dysfunction and eccentric vessel growth (positive remodeling) 1, which leads to progressive obstruction of the lumen due to the growth of atheromatous plaques.
Significant obstruction of arteries, particularly the coronary tree, can be defined in different ways. From a functional standpoint, ischemia is defined as the inability to furnish adequate blood flow in situations of increased demand such as exertion or intravenous adenosine administration, despite the self-regulatory mechanisms of the microvasculature. This generally occurs when there is ≥50 % stenosis, which can give rise to symptoms and is thus of clinical significance. Functional assessment can be by non-invasive (exercise testing, stress echocardiography, myocardial perfusion scintigraphy, or magnetic resonance perfusion study) or invasive means (intracoronary Doppler or calculation of FFR) 2,3. The latter method, recently validated in two large clinical trials, DEFER 4 and FAME 5, assesses the functional significance of a coronary lesion. FFR is the ratio between the pressures downstream (distal vessel pressure) and upstream (aortic pressure) of the lesion measured at maximal hyperemia, obtained by administration of intracoronary adenosine (a vasodilator) in bolus or perfusion. The technique can assess isolated or sequential lesions and thus identify which lesions are causing the ischemia.
The arterial lumen can be assessed anatomically by angiography, which is considered the gold standard for determining the presence and extent of disease, although recent advances in multislice computed tomography may provide a valid alternative. Over 75 % obstruction is considered significant. However, assessment of the lumen, even in various planes and using computer-assisted quantitative coronary angiography (QCA), can lead to two types of error. It can overestimate the significance of an intermediate lesion that does not cause functional ischemia, resulting in unnecessary percutaneous treatment. The FAME trial showed that percutaneous coronary intervention (PCI) guided by FFR in patients with multivessel disease led to a significant reduction in major adverse cardiac events at one-year (76 vs. 113, p <0.02) and two-year follow-up (105 vs. 141, p <0.01), compared to PCI guided by angiography only, with a parallel reduction in the number of stents used per patient (1.9 vs. 2.7, p <0.001), procedure time and length of hospital stay 5. More recently, a substudy of the same trial, analyzing the functional significance of lesions according to the degree of angiographic stenosis, concluded that 65 % of lesions classified as 50-70 % and 20 % of those classified as 70-90 % were not functionally significant 6.
On the other hand, angiography, being a luminographic technique, may underestimate the significance of a plaque, since it does not assess the vessel wall and the contribution of positive remodeling 7. Improved understanding of the pathophysiology of atherosclerosis has shown that two-thirds of acute coronary syndromes are caused by functionally and/or angiographically non-significant atheromas plaques becoming unstable and thus clinically significant 8.
The difficulty of assessing the significance of coronary disease is sometimes evident during catheterization, as in the case presented, when it affected treatment. Based on current knowledge, angiographic assessment of lesions of intermediate significance (50-70 %) should be complemented by functional assessment using FFR. A value of <0.80 justifies treating the lesion, while a value of ≥0.80 does not. Until the publication of the FAME study, values between 0.76 and 0.79 were considered to be a gray area, in which treatment was not considered obligatory 9.
Histological study of the vessel wall using IVUS can add vital information 10, even in the absence of functional assessment 11. Through direct visualization of the vessel wall and its different layers, IVUS can determine the size, distribution (including in bifurcations and ostia), and constitution (particularly calcium content) of atheromatous plaques. Studies correlating luminal area by IVUS and functional repercussions show that lesions are significant when the area is <6mm 2 in the left main artery or <4mm 2 in any other native vessel. This guides the choice of treatment strategy, as well as the need for lesion preparation (plaque modification techniques such as directional, rotational and cutting balloon atherectomy) before stent placement, and the selection of appropriately sized stents. IVUS can also be used to evaluate treatment outcomes, including identifying dissections and thrombi, and confirming correct stent apposition and expansion. 12,13. In the case presented, IVUS following the first overdilation of the Endeavor drug-eluting stent detected the stent's underexpansion, a factor which can have negative repercussions (exemplified by the in-stent occlusion in 2004), and enabled subsequent correction, resulting in a luminal area of >9mm 2.
ConclusionThe significance of a coronary lesion, naturally taking into account the patient's symptoms, should be determined on the basis of information provided by careful selection of the different diagnostic methods available, which will help to avoid errors of judgement and thus improve treatment.
Coronary angiography has traditionally been the gold standard for classifying coronary lesions, but is now giving way to a series of techniques that go beyond luminography. Methods are now available to assess plaque characteristics (IVUS) and functional repercussions (FFR), which can be used to determine indications for mechanical intervention and to evaluate its outcome. Together, these techniques, which complement conventional angiography, are becoming established as the most important determinants of the success of percutaneous coronary intervention.
