
A 69-year-old man was admitted with chest pain lasting for four days. The electrocardiogram showed ST elevation in the inferior leads, with Q waves and inverted T waves.
He was taken for urgent cardiac catheterization, which showed 3-vessel disease, with thrombotic occlusion of the right coronary artery. Angioplasty with a bare metal stent was performed.
The patient rapidly evolved with cardiogenic shock and a new systolic murmur.
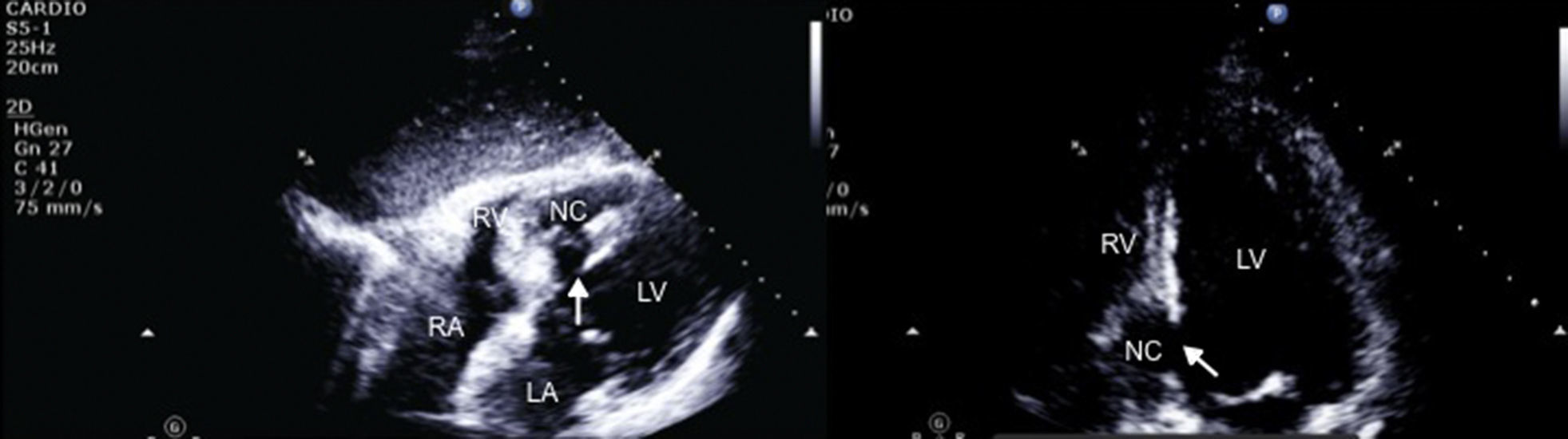
The echocardiogram revealed interventricular septal rupture with an extensive interventricular communication at the level of the posterobasal septum, associated with a serpiginous dissection of the septum, forming a neocavity, with an exit port in the mid-apical area of the right ventricle (Figure 1). Akinesis of the basal half of the inferior and posterior wall was also evident.
 and apical 4-chamber view, zoom on the left ventricle (right). Rupture of the interventricular septum, with septal dissection. LA: left atrium; LV: left ventricle; NC: neocavity formed by the dissection of the interventricular septum; RA: right atrium; RV: right ventricle. Arrow: interventricular septal rupture.")
Transthoracic echocardiography, subcostal (left) and apical 4-chamber view, zoom on the left ventricle (right). Rupture of the interventricular septum, with septal dissection. LA: left atrium; LV: left ventricle; NC: neocavity formed by the dissection of the interventricular septum; RA: right atrium; RV: right ventricle. Arrow: interventricular septal rupture.
An intra-aortic balloon pump was placed and the patient was sent for emergent surgery. The interventricular septal rupture was closed using a pericardial patch and excluding the infarcted area.
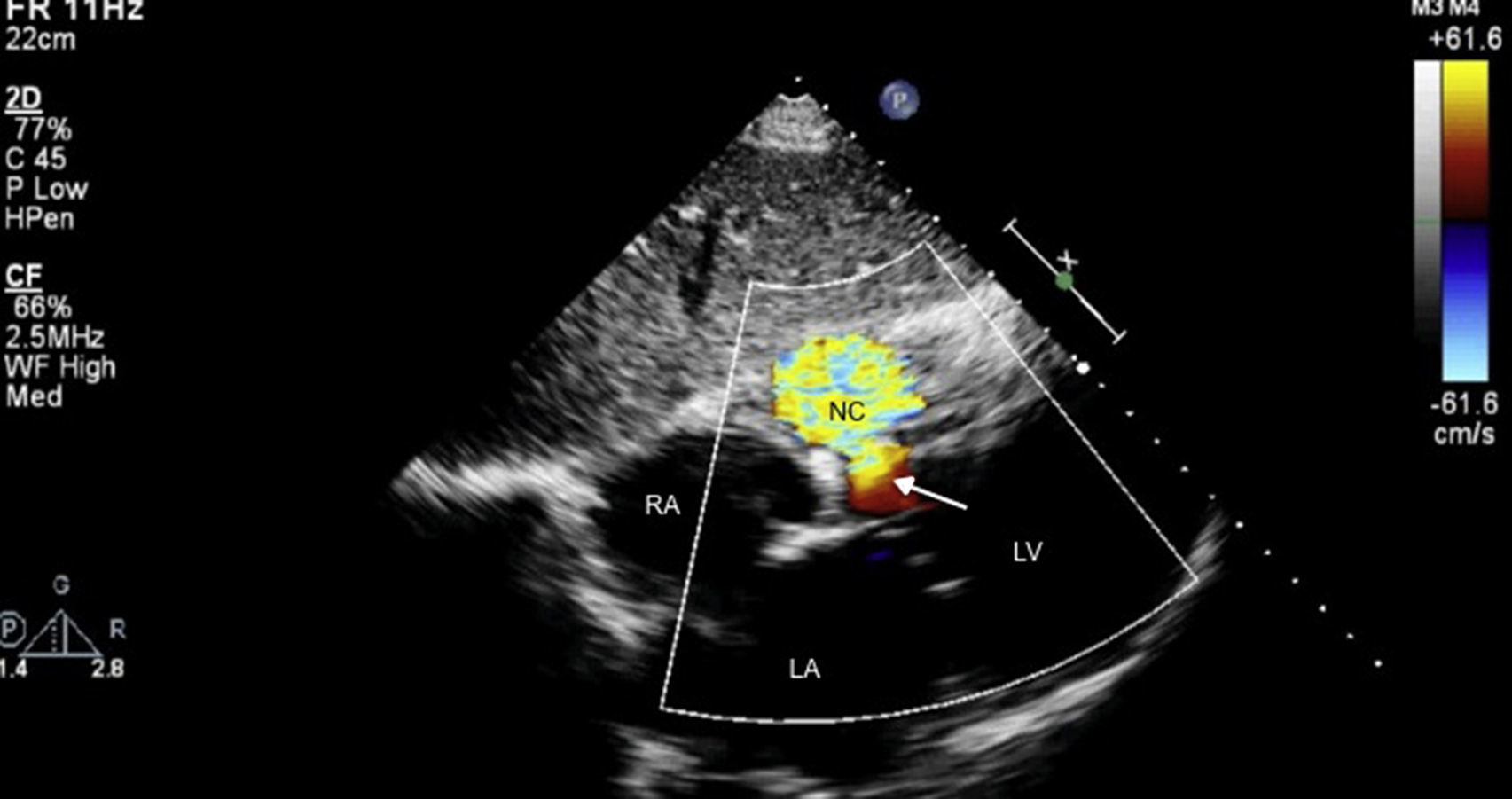
Although the patch significantly reduced the interventricular communication, a residual defect remained, with turbulent left-to-right shunt, draining into a cavity that corresponded to the aneurysmal dissection of the septum, and that communicated distally with the right ventricle (Figure 2), findings confirmed by cardiac magnetic resonance imaging (Figures 3 and 4).

Transthoracic echocardiography, subcostal view. After surgery, an interventricular communication remains, with left-to-right shunt. LA: left atrium; LV: left ventricle; NC: neocavity formed by the dissection of the interventricular septum; RA: right atrium. Arrow: interventricular septal rupture.
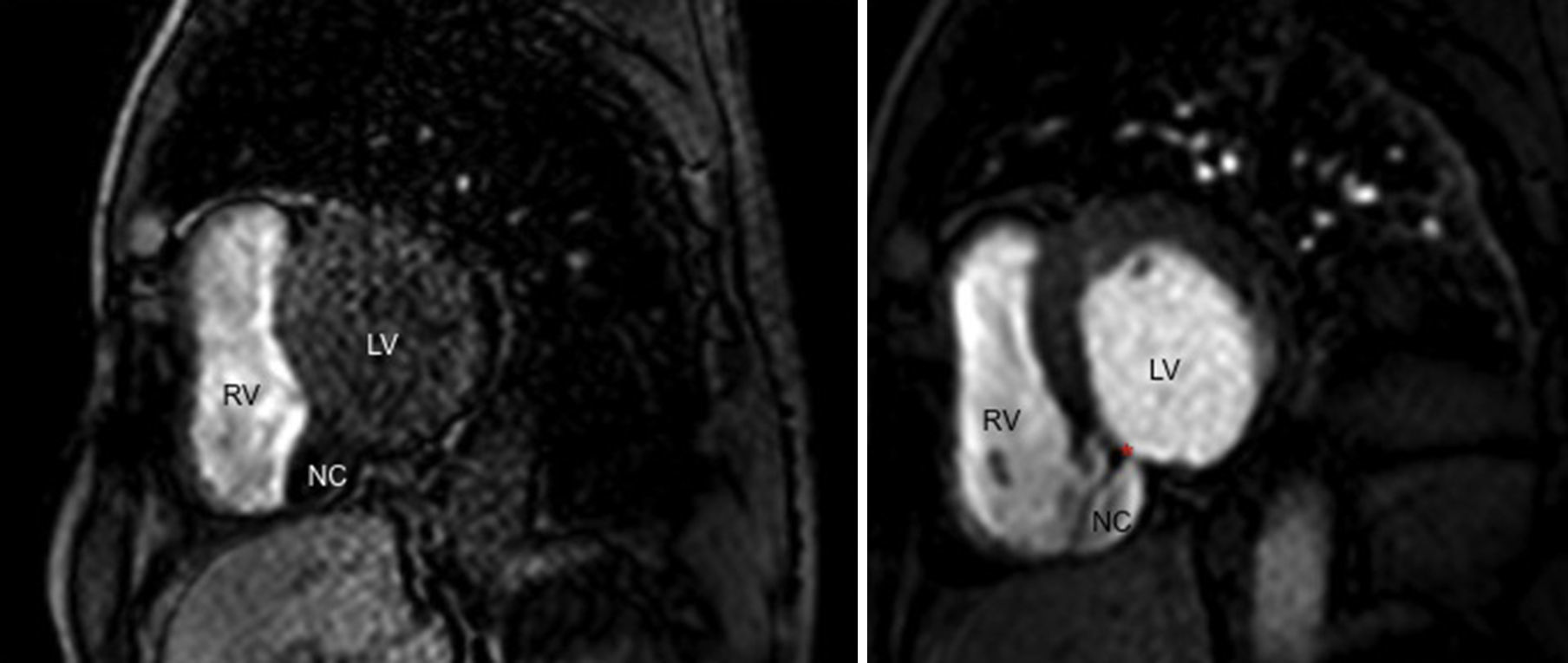
, short-axis view at the level of the basal ventricular segments. There is a residual defect in the posterior interventricular septum, communicating with a neocavity formed by the aneurysmal dissection of the septum. LV: left ventricle; NC: neocavity formed by the dissection of the interventricular septum; RV: right ventricle. Arrow: interventricular septal rupture; asterisk: residual ventricular septal defect.")
Cardiac magnetic resonance image from cine balanced steady-state free procession sequences (bright blood), short-axis view at the level of the basal ventricular segments. There is a residual defect in the posterior interventricular septum, communicating with a neocavity formed by the aneurysmal dissection of the septum. LV: left ventricle; NC: neocavity formed by the dissection of the interventricular septum; RV: right ventricle. Arrow: interventricular septal rupture; asterisk: residual ventricular septal defect.

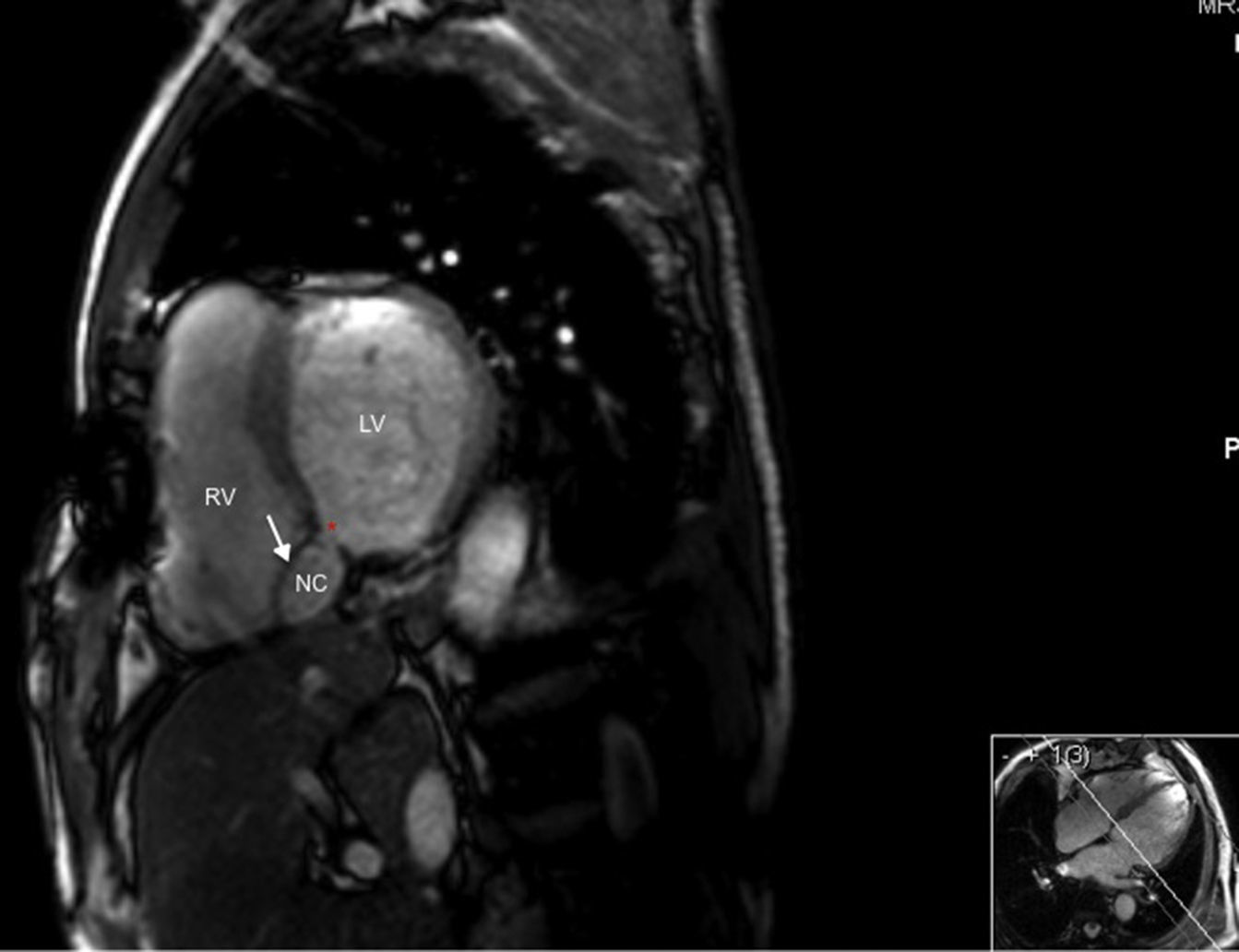
Cardiac magnetic resonance gadolinium perfusion imaging. Immediately after contrast injection, flow can be seen from the left ventricle into the cavity formed by the interventricular septal dissection, which finally drains into the apical region of the right ventricle. LV: left ventricle; NC: neocavity formed by the dissection of the interventricular septum; RV: right ventricle. Asterisk: residual ventricular septal defect.
This is an interesting case of an uncommon and catastrophic mechanical complication of myocardial infarction1–5 which illustrates the decisive role that echocardiography can play in guiding the heart team through diagnosis and follow-up.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
