
The association between exercise and coronary atherosclerosis still remains unclarified. We aimed to analyze the prevalence of high coronary atherosclerotic burden in veteran athletes, considering cardiovascular (CV) risk and volume of exercise.
MethodsA total of 105 asymptomatic male veteran athletes (48±5.6 years old) were studied. A high coronary atherosclerotic burden was defined as one of the following characteristics in coronary computed tomography angiography: calcium score >100, >75th percentile, obstructive plaques, involving left main, three-vessels or two-vessels including proximal anterior descending artery, segment involvement score >5 or CT-adapted Leaman score ≥5. CV risk was stratified by SCORE2 and volume of exercise by metabolic equivalent task score.
ResultsMost athletes (n=88) were engaged in endurance sports for 17.1±9.8 years, with a median exercise volume of 66 [IQR 44–103] metabolic equivalent of tasks/hour/week. The mean Systematic Coronary Risk Evaluation 2 was 2.8±1.5%; 76.9% of athletes had a low-moderate risk and none a very high risk. High coronary atherosclerotic burden was present in 25.7% athletes. Athletes with high cardiovascular risk and high exercise volume (above the median) showed significantly high coronary atherosclerotic burden compared to those with low-moderate risk and high volume (50.0% vs. 15.6%; p=0.017). Among athletes with low to moderate risk, a high volume of exercise tended to be protective, while in those with low volume, there was similar rate of high coronary atherosclerotic burden, regardless of CV risk.
ConclusionsA combination of higher volume of exercise and high cardiovascular risk revealed the worst association with coronary atherosclerosis in veteran athletes. The relationship between these variables is controversial, but integrating exercise characteristics and risk assessment into preparticipation evaluation is essential.
A associação entre exercício e aterosclerose coronária permanece pouco esclarecida. O nosso objetivo foi analisar a prevalência de alta carga aterosclerótica coronária (CASC) em atletas veteranos, integrando o risco cardiovascular (RCV) e volume de exercício.
MétodosAvaliámos 105 atletas veteranos, homens assintomáticos (48±5,6 anos). Alta CASC foi definida como uma das: score de cálcio >100, >percentil 75, placas obstrutivas, envolvimento do tronco da artéria coronária esquerda, doença de 3 vasos ou 2 vasos incluindo artéria descendente anterior proximal, Segment Involvement Score >5 ou Score Leaman adaptado por CT ≥5. Estratificámos o RCV pelo SCORE2 e o volume de exercício por equivalentes metabólicos (METs).
ResultadosA maioria dos atletas (n=88) praticava desportos de resistência, durante 17,1±9,8 anos, com um volume de exercício mediano de 66 [IQR 44-103] METs/hora/semana. O SCORE2 médio foi 2,8±1,5% e 76,9% dos atletas tinham RCV baixo-moderado e nenhum RCV muito-alto. Alta CASC ocorreu em 25,7%. Atletas com alto RCV e alto volume de exercício (acima da mediana) apresentaram CASC significativamente alta em comparação com os com RCV baixo-moderado e alto volume (50,0% versus 15,6%; p=0,017). Nos atletas com RCV baixo-moderado, o alto volume de exercício mostrou uma tendência protetora, enquanto houve uma taxa semelhante de alta CASC naqueles com baixo volume, independentemente do RCV.
ConclusõesEm atletas veteranos, a combinação de maior volume de exercício com alto RCV mostrou a pior associação com aterosclerose coronária. A relação entre estas variáveis é controversa, mas integrar características do exercício e o RCV na avaliação pré-participação é essencial.
Regular physical activity and exercise training have several well-known positive effects on health. As cardiovascular (CV) diseases remain the worldwide leading cause of death, mostly due to atherosclerotic coronary artery disease (CAD), the promotion of a healthy lifestyle is a cornerstone of CV prevention. Exercise is associated with a lower risk of major clinical events, including death, stroke and myocardial infarction, better blood pressure regulation, favorable lipid profile and reduced incidence of diabetes.1
The engagement of middle-aged individuals in organized sports activities, particularly in endurance sports, has progressively increased in the last decade, at a recreational and competitive level. This presents new challenges for medical evaluation and sports eligibility. Despite the multiple protective effects of exercise, CAD is the most frequent cause of sudden cardiac death among veteran athletes, accounting for approximately two-thirds of all cases.2–5 In this setting, preparticipation screening methodologies applied to middle-aged athletes should focus on CV risk stratification and early detection of CAD.6
Several studies have suggested a potential paradoxical link between lifelong endurance exercise and coronary atherosclerosis. In fact, when compared to healthy sedentary individuals, these athletes have higher coronary artery calcium (CAC) scores and prevalence of overall coronary plaques.2–4 Underlying mechanisms for this interaction remain elusive and have spurred debate about a potential selection bias in these series, age-related differences, prior presence of CV risk factors and the potential effect of exercise-related factors.7 Otherwise, the clinical relevance of this association between volume of exercise and development of coronary atherosclerosis in veteran athletes remains unknown. Nevertheless, it is well-established that CAC score holds significant prognostic value in general population, especially in individuals with intermediate risk, compared to conventional clinical risk factors.8
Furthermore, emerging literature has described relative distinctions in plaque composition, with athletes exhibiting a predilection for more stable (calcified) plaques than non-athletes, in whom plaque morphology often manifests as mixed.9,4,5 These differences in plaque composition hypothesize that its more stable profile in athletes could be potentially associated with a lower rate of rupture and subsequent acute coronary events. However, a recent study showed a higher prevalence of coronary plaques, including non-calcified and mixed types, as well as plaques in proximal segments with significant luminal stenosis, in middle-aged athletes compared to fit and healthy individuals, with a similarly low CV risk profile.10
Considering these new insights and controversial data, it is crucial to clarify the relationship between lifelong endurance exercise and coronary atherosclerosis, especially using advanced imaging tools and new available clinical risk scores. Additionally, as is the case in the general middle-aged population, the rising number of veteran athletes includes a heterogenous population regarding CV risk profile, traditionally excluded from the previous studies, that in clinical practice are evaluated using the recommended clinical risk scores.
ObjectivesThe aim of this study was to analyze the prevalence of high coronary atherosclerotic burden in veteran athletes, assessed by coronary computed tomography angiography (CCTA), considering the CV risk stratified by Systematic Coronary Risk Evaluation 2 (SCORE2) and the volume of exercise.
MethodsStudy design and populationVeteran male asymptomatic athletes aged ≥40 years old, participating in regular exercise for at least four hours a week, for a minimum of consecutive five years, were enrolled in this prospective observational study. Previous known CV disease, renal impairment, diabetes, and allergy to iodinated contrast agents were exclusion criteria. The initial assessment regarding sports eligibility was performed in a dedicated sports cardiology clinic and included physical examination, documentation of demographics, anthropometric characteristics, CV risk factors and sports history, blood tests, 12-lead resting electrocardiogram, transthoracic echocardiogram, and exercise testing. CV risk was determined according to the SCORE211 and the athletes were distributed by the correspondent risk classes (low to moderate risk: SCORE2 <2.5% if age <50 years old or SCORE2 <5% if age 50–69 years old; high risk: SCORE2 2.5–7.4% if age <50 years old or SCORE2 5–9.9% if age 50–69 years old; very high risk: SCORE2 ≥7.5% if age <50 years old or SCORE2 ≥10% if age 50–69 years old).12 For the purpose of this analysis, the population was subdivided into two groups according to CV risk: low to moderate and high risk. The study was approved by the ethics committee and all individuals gave their informed consent for participation.
Exercise assessmentA detailed characterization of the sports disciplines and exercise practice was performed, including the Mitchell classification.13 Exercise volume was determined by the metabolic equivalent of task (MET) score (METs/hours/week), calculated as the product of intensity, frequency and duration of exercise. Exercise intensity was defined by the METs for each reported sport according to the Compendium of Physical Activities,14 frequency by the number of training sessions per week and duration by the number of hours spent on each workout. The studied population was stratified into two groups according to the median of exercise volume: below vs. above the median of volume exercise.
Coronary computed tomography angiographyCoronary atherosclerotic burden was determined by CAC score and CCTA, using multidetector (≥64-slice) CT scanners (SOMATOM Force and SOMATOM Perspective, Siemens Healthcare Inc.). Except when contraindicated, sublingual nitroglycerin (0.5 mg) was administered, and beta-blockers were used when appropriate (heart rate >65 bpm). A cardiologist and a radiologist with level III-equivalent experience analyzed all scans, which were processed on a workstation (syngo.via, Siemens Healthcare Inc.). CAC scores were expressed in absolute values and percentiles adjusted for age, gender, and ethnicity. The presence of coronary plaque, plaque morphology, distribution (Society of Cardiovascular Computed Tomography classification)15 and degree of stenosis were ascertained with CCTA to calculate the segment involvement score (SIS) and CT Leaman score (CT-LeSc).16–18 A significant SIS was considered if >5 segments involved. CT-LeSc was calculated from three sets of weighting factors: (1) location of plaques in the coronary tree, taking dominance into account; (2) type of plaque; (3) degree of stenosis.17 CT-LeSc ≥5 was defined as significant. A higher atherosclerotic burden was established as the presence of at least one of the following characteristics: CAC score >100 Agatston units (AU); CAC score>75th percentile; obstructive CAD (≥50% luminal stenosis); presence of plaques in the left main (LM), 3-vessels or 2-vessels involving the proximal left anterior descending artery (LAD); SIS >5; or CT-LeSc ≥5.
Statistical analysisStatistical analysis was performed using IBM SPSS for Windows version 29.0 (IBM SPSS, Inc., Chicago, IL). Normality was tested with the Kolmogorov–Smirnov test. Continuous variables with normal distribution were expressed as means and standard deviation and non-normal variables as median (interquartile range). Categorical variables were expressed as frequencies and percentages. Statistical comparisons were performed using the chi-square test or Fisher's exact test, when appropriate, for categorical variables, and the Mann–Whitney or Kruskal–Wallis test for continuous variables. A p value <0.05 was considered statistically significant.
ResultsBaseline characteristics and CV riskDemographic and clinical characteristics are presented in Table 1, while in Table 2 the characteristics associated with CV risk are illustrated. Of the 105 athletes included, the great majority (n=103; 98.1%) were Caucasian, with a mean age of 48±6 years old.
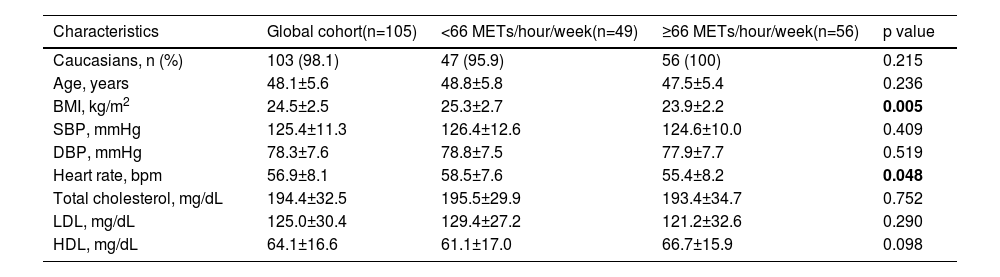
Demographic and clinical characteristics.
| Characteristics | Global cohort(n=105) | <66 METs/hour/week(n=49) | ≥66 METs/hour/week(n=56) | p value |
|---|---|---|---|---|
| Caucasians, n (%) | 103 (98.1) | 47 (95.9) | 56 (100) | 0.215 |
| Age, years | 48.1±5.6 | 48.8±5.8 | 47.5±5.4 | 0.236 |
| BMI, kg/m2 | 24.5±2.5 | 25.3±2.7 | 23.9±2.2 | 0.005 |
| SBP, mmHg | 125.4±11.3 | 126.4±12.6 | 124.6±10.0 | 0.409 |
| DBP, mmHg | 78.3±7.6 | 78.8±7.5 | 77.9±7.7 | 0.519 |
| Heart rate, bpm | 56.9±8.1 | 58.5±7.6 | 55.4±8.2 | 0.048 |
| Total cholesterol, mg/dL | 194.4±32.5 | 195.5±29.9 | 193.4±34.7 | 0.752 |
| LDL, mg/dL | 125.0±30.4 | 129.4±27.2 | 121.2±32.6 | 0.290 |
| HDL, mg/dL | 64.1±16.6 | 61.1±17.0 | 66.7±15.9 | 0.098 |
Bbold number are the values: statistical significance (p<0.05).
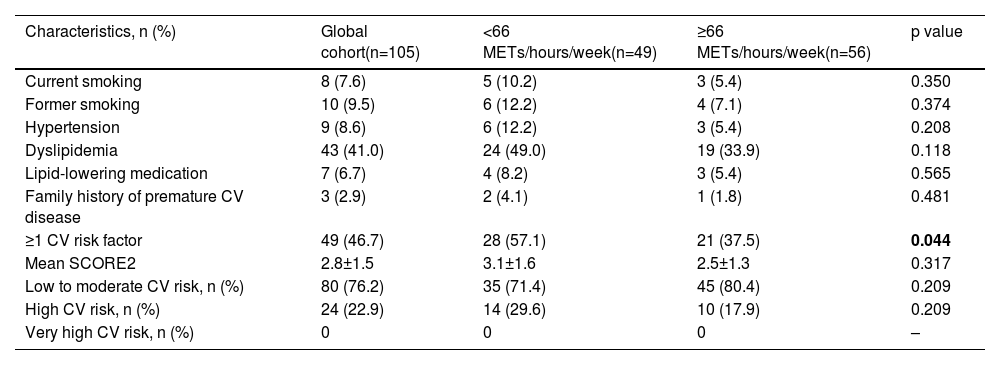
Cardiovascular risk.
| Characteristics, n (%) | Global cohort(n=105) | <66 METs/hours/week(n=49) | ≥66 METs/hours/week(n=56) | p value |
|---|---|---|---|---|
| Current smoking | 8 (7.6) | 5 (10.2) | 3 (5.4) | 0.350 |
| Former smoking | 10 (9.5) | 6 (12.2) | 4 (7.1) | 0.374 |
| Hypertension | 9 (8.6) | 6 (12.2) | 3 (5.4) | 0.208 |
| Dyslipidemia | 43 (41.0) | 24 (49.0) | 19 (33.9) | 0.118 |
| Lipid-lowering medication | 7 (6.7) | 4 (8.2) | 3 (5.4) | 0.565 |
| Family history of premature CV disease | 3 (2.9) | 2 (4.1) | 1 (1.8) | 0.481 |
| ≥1 CV risk factor | 49 (46.7) | 28 (57.1) | 21 (37.5) | 0.044 |
| Mean SCORE2 | 2.8±1.5 | 3.1±1.6 | 2.5±1.3 | 0.317 |
| Low to moderate CV risk, n (%) | 80 (76.2) | 35 (71.4) | 45 (80.4) | 0.209 |
| High CV risk, n (%) | 24 (22.9) | 14 (29.6) | 10 (17.9) | 0.209 |
| Very high CV risk, n (%) | 0 | 0 | 0 | – |
Overall, 46.7% athletes exhibited at least one CV risk factor. The most prevalent risk factor was dyslipidemia, present in 43 (41.0%) athletes, with a mean LDL cholesterol level of 125.0±30.4 mg/dL, and seven athletes (6.7%) were under lipid-lowering therapy. The mean body mass index (BMI) was 24.5±2.5 kg/m2 and 18 (17.1%) athletes were current or former smokers. The mean SCORE2 was 2.8±1.5% and most of athletes (76.2%) had low to moderate CV risk, while none had very high risk.
When the athletes were stratified according to the median volume of exercise (66 METs/hours/week), demographic and clinical profiles were overall similar across both groups (below vs. above the median), including the mean SCORE2 (3.1±1.6% vs. 2.5±1.3%; p=0.317). However, the subgroup of athletes with less volume of exercise had significantly higher prevalence of at least one CV risk factor (57.1% vs. 37.5%; p=0.044) and a significantly higher mean BMI (25.3±2.7 kg/m2 vs. 23.9±2.2 kg/m2; p=0.005), compared to those practicing a larger volume of exercise.
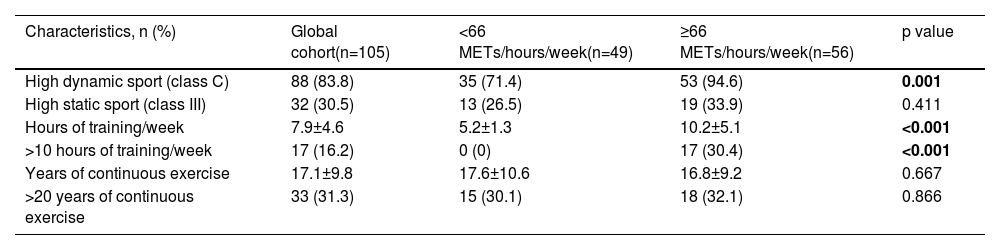
Exercise-related characteristicsExercise-related characteristics are shown in Table 3. Most athletes (n=88; 83.8%) were engaged in endurance sports, especially running (n=67) and cycling (n=11), a quarter (24.8%) at competitive level. The mean number of years of continuous exercise training was 17.1±9.8 years, with 7.9±4.6 hours of training per week and a median volume of 66 [IQR 44–103] METs/hours/week. The subgroup of athletes with higher volume of exercise training (above the median) were significantly more involved in high dynamic sport (class C) (94.6% vs. 71.4%; p=0.001) and trained more hours per week (10.2±5.1 hours vs. 5.2±1.0 hours; p<0.001).
Exercise-related characteristics.
| Characteristics, n (%) | Global cohort(n=105) | <66 METs/hours/week(n=49) | ≥66 METs/hours/week(n=56) | p value |
|---|---|---|---|---|
| High dynamic sport (class C) | 88 (83.8) | 35 (71.4) | 53 (94.6) | 0.001 |
| High static sport (class III) | 32 (30.5) | 13 (26.5) | 19 (33.9) | 0.411 |
| Hours of training/week | 7.9±4.6 | 5.2±1.3 | 10.2±5.1 | <0.001 |
| >10 hours of training/week | 17 (16.2) | 0 (0) | 17 (30.4) | <0.001 |
| Years of continuous exercise | 17.1±9.8 | 17.6±10.6 | 16.8±9.2 | 0.667 |
| >20 years of continuous exercise | 33 (31.3) | 15 (30.1) | 18 (32.1) | 0.866 |
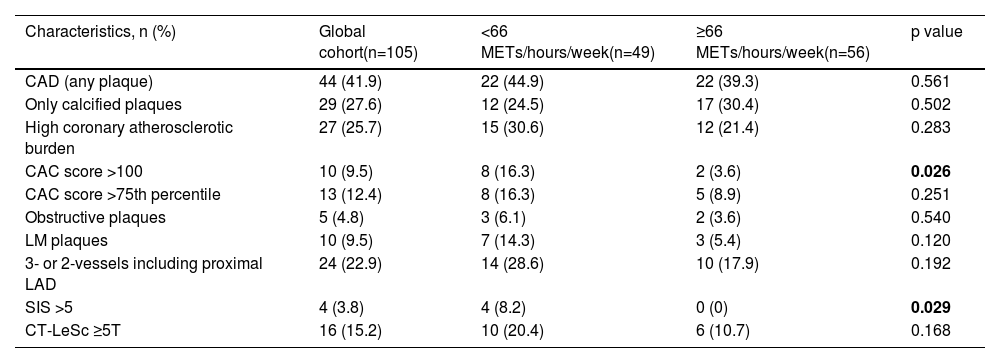
A detailed analysis of the CCTA results is presented in Table 4.
CCTA data.
| Characteristics, n (%) | Global cohort(n=105) | <66 METs/hours/week(n=49) | ≥66 METs/hours/week(n=56) | p value |
|---|---|---|---|---|
| CAD (any plaque) | 44 (41.9) | 22 (44.9) | 22 (39.3) | 0.561 |
| Only calcified plaques | 29 (27.6) | 12 (24.5) | 17 (30.4) | 0.502 |
| High coronary atherosclerotic burden | 27 (25.7) | 15 (30.6) | 12 (21.4) | 0.283 |
| CAC score >100 | 10 (9.5) | 8 (16.3) | 2 (3.6) | 0.026 |
| CAC score >75th percentile | 13 (12.4) | 8 (16.3) | 5 (8.9) | 0.251 |
| Obstructive plaques | 5 (4.8) | 3 (6.1) | 2 (3.6) | 0.540 |
| LM plaques | 10 (9.5) | 7 (14.3) | 3 (5.4) | 0.120 |
| 3- or 2-vessels including proximal LAD | 24 (22.9) | 14 (28.6) | 10 (17.9) | 0.192 |
| SIS >5 | 4 (3.8) | 4 (8.2) | 0 (0) | 0.029 |
| CT-LeSc ≥5T | 16 (15.2) | 10 (20.4) | 6 (10.7) | 0.168 |
In total, 44 (41.9%) athletes presented coronary plaques and approximately a quarter had a high coronary atherosclerotic burden (n=27; 25.7%). CAC score >100 was present in 10 (9.5%) and CAC score >75th percentile in 13 (12.4%) athletes. Most of the plaques were calcified in nature (85.7%), while the rate of mixed plaques was 11.4% and of non-calcified was 2.9%. In relation to the degree of the coronary stenosis, 36 (34.3%) plaques were non-obstructive and 5 (4.8%) were obstructive. The frequency of athletes with three-vessels or two-vessels involving the proximal LAD was 22.9%, SIS >5 3.8% and CT-LeSc ≥5 15.2%.
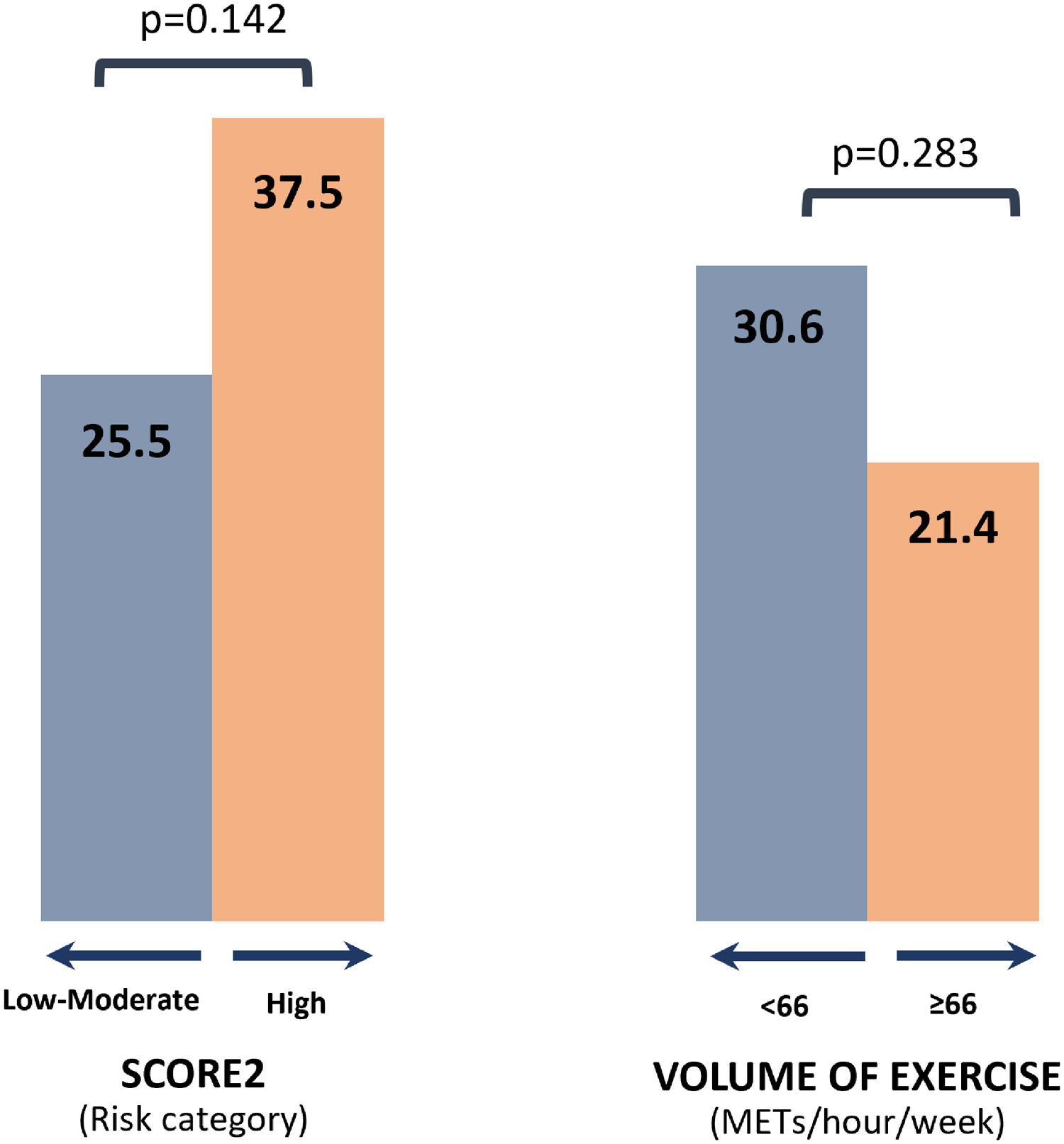
According to the volume of exercise, athletes exercising <66 METs/hours/week had a CAC score more frequently >100 (16.3% vs. 3.6%; p=0.026) and SIS >5 (8.2% vs. 0.0%; p=0.029), compared with the subgroup with higher volume of exercise. The presence of high coronary atherosclerotic burden was similar between these two groups [below vs. above median: 30.6% vs. 21.4%, respectively; p=0.283] and was also not significantly different according to the SCORE2 risk categories [low to moderate vs. high risk: 25.5% vs. 37.5%; p=0.142] (Figure 1). Additionally, in the studied population, high coronary atherosclerotic burden was not significantly different according to the presence (vs. absence) of the following characteristics: at least one CV risk factor (22.4% vs. 28.6%; p=0.474), dyslipidemia (25.6% vs. 25.8%; p=0.979), and current/former smoking (11.1% vs. 28.7%; p=0.119).

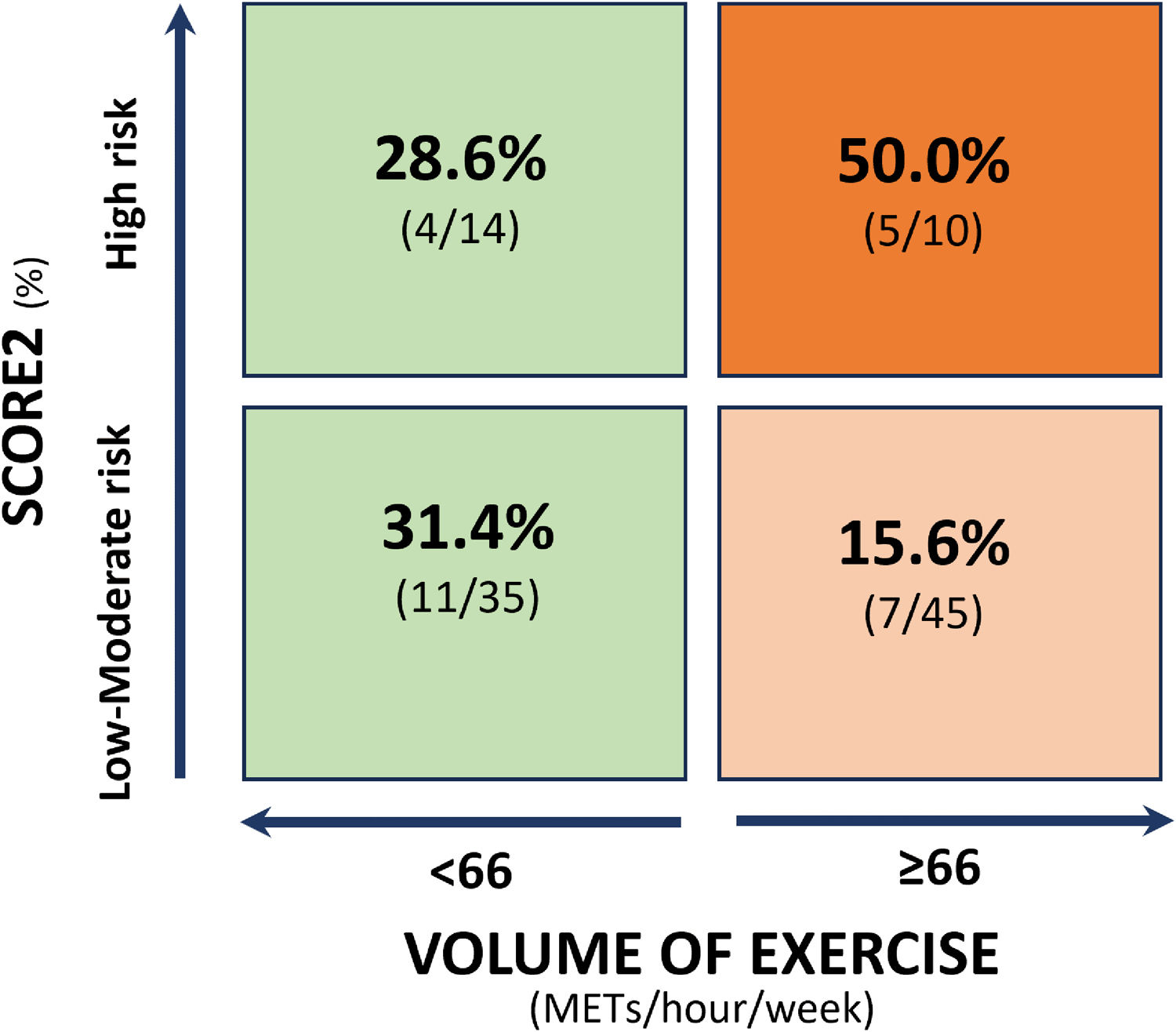
Combining the variables “volume of exercise” and “CV risk class”, those athletes with high CV risk and high volume of exercise showed a significantly higher rate of a high coronary atherosclerotic burden compared to those with low to moderate risk and high volume of exercise (50.0% vs. 15.6%; p=0.017). Among athletes with low to moderate risk, high volume of exercise trended to be protective (15.6% vs. 31.4%; p=0.092), while there was a similar rate of high coronary atherosclerotic burden in athletes with low volume of exercise, regardless of risk class (Figure 2).
Discussion
The present study conducted in veteran male athletes demonstrates the complex interaction between exercise, CV risk and coronary atherosclerotic evaluated by CCTA. One fourth of the athletes had high coronary atherosclerotic burden, which was more frequent in those combining high volume of exercise with high CV risk, while among athletes with low to moderate risk, exercising with a higher volume tended to be protective. Integrating clinical and exercise-related characteristics during the preparticipation evaluation of middle-aged individuals is crucial.
Regular physical exercise is protective in patients with CAD, whereas minimal or physical inactivity substantially increases the clinical risk.12 Nevertheless, a higher-than-expected coronary calcification has been reported in multiple studies with veteran athletes engaged in lifelong endurance exercise, compared to their non-athlete counterparts. We also described a high incidence of subclinical CAD in veteran athletes, without significant correlation between duration or intensity of exercise and extent or severity of CAD.19 In the present analysis, 41.9% of the athletes had at least one coronary plaque, mainly calcified, what is aligned with previous reports, showing that athletes have a higher likelihood of calcified plaques, while non-athletes have more commonly mixed plaques.5,9,4 The potential clinical relevance of these plaques in athletes remains unknown, but it has been advocated that this composition confers greater stability, leading to lower rate of future acute coronary clinical events.
However, some studies have revealed different and controversial data about this relationship between exercise and CAD. A prospective single-site study of recreational endurance athletes showed an inverse proportion of coronary atherosclerosis burden, stenosis severity and high-risk plaque features, with the frequency and duration of exercise, with regular moderate-to-high exercise resulting in lower total and non-calcified plaques and less high-risk plaques.20 The recent Master@Heart study also provided additional insights, comparing 191 lifelong master endurance athletes, 191 late-onset athletes and 176 healthy non-athletes, all male with low CV risk. In fact, contrary to prior expectations, this study showed that lifelong endurance athletes did not exhibit a more favorable coronary plaque composition compared to healthy non-athletes. Specifically, lifelong endurance athletes had a higher prevalence of coronary plaques, including a greater proportion of non-calcified plaques in proximal segments. The authors suggest a possible reverse J-shaped dose-response relationship between endurance training and coronary atherosclerosis.10
Some of the methodological aspects adopted in our study differ from earlier studies, partially justifying the results. The selected population seems to better represent most of the middle-aged athletes followed in daily clinical practice. This growing number of individuals, involved in lifelong regular exercise training, mostly at recreational level and without know CV disease, may already have some conventional risk factors, such as in the general population. The great majority of the athletes included in our study had low to moderate CV risk, but 46.7% had at least one CV risk factor, especially dyslipidemia and past/present smoking. The SCORE2 was not significantly different according to the volume of exercise, but the subgroup of athletes with less volume of exercise had higher prevalence of at least one CV risk factor, what is in accordance with the well-known benefits of exercise in control and prevention of risk factors. Such as in previous studies, it is important to stress that no athlete had very high CV risk, but in our study, beyond diabetes, the CV risk factors were not exclusion criteria. These differences in baseline characteristics, especially the CV risk profile, limit direct comparisons and generalization of the results. For example, in the Master@Heart10 study, individuals with CV risk factors were excluded. Interestingly, the median levels of LDL cholesterol were similar. Also compared to this study, our cohort included younger individuals, with less training volume, fewer hours of training per week and fewer years of training. In the Master@Heart study all athletes practiced endurance training, of which cycling was the most common, while in our study 83.8% were involved in endurance sports, of which running was the most common.
In our study, the evaluation of coronary atherosclerosis by CCTA was more detailed when compared to other analyses. Beyond CAC score, degree of coronary stenosis and plaques composition, we also applied validated angiographic scores and one variable of high coronary atherosclerosis burden was defined, including these characteristics with proven prognostic a clinical impact. The presence of high coronary atherosclerotic burden was similar across the volume of exercise and the SCORE2 categories. This variable was not only tested isolated, but also combining the volume of exercise and the CV risk. The only inclusion of veteran athletes (no sedentary or inactive individuals), being differentiated by the volume of exercise (below and above the median) and the CV risk stratified by the recent recommended SCORE2, are also aspects not previously analyzed. To our knowledge this is the first study integrating CV risk calculated through the SCORE2 with the training volume, being important to test this association in different and large populations of athletes.
Interestingly, despite the absence of significant differences in the prevalence of high coronary atherosclerotic burden between athletes with low to moderate CV risk and those with high CV risk, a relevant association emerged when considering the volume of exercise. Specifically, when integrating the SCORE2 risk categories with the volume of exercise, we found that athletes with high CV risk and high volume of exercise revealed significantly higher occurrence of atherosclerosis compared to those with low to moderate risk and high volume of exercise. These findings suggest a potential synergistic effect between CV risk and exercise on coronary plaque formation and progression. On the other hand, athletes at low to moderate CV risk and engaged in high volume of exercise trended toward a protective effect. Conversely, there was a comparable incidence of a high coronary atherosclerotic burden among athletes with lower exercise volume, regardless of their risk classification. These findings suggest a complex relationship between exercise volume, CV risk, and coronary atherosclerosis and underscores the importance of considering together the individual exercise habits and CV risk profiles when assessing the coronary atherosclerotic risk in clinical practice.
The limitations of the present study include the relatively small sample size, which may limit the generalization of our findings. The cross-sectional nature precludes the establishment of causality and temporality between exercise, CV risk and coronary atherosclerotic burden. Additionally, the population comprised exclusively endurance male athletes, limiting the generalization to other populations. Moreover, the reliance on self-reported exercise habits may introduce recall bias and inaccuracies in exercise volume assessment. Even excluding athletes with previous known CV diseases and the majority having low to moderate CV risk, inclusion of individuals with factors such as dyslipidemia and smoking can make the interpretation of the results more difficult. Lastly, we did not test for the use of performance-enhancing agents that may influence some results.
Overall, our study emphasizes the need for personalized risk assessment and tailored exercise recommendations in veteran male athletes to reduce CV risk. Indeed, there is no current data indicating an increased risk of ischemic heart disease events in endurance athletes, while the most compelling evidence suggests that engaging in regular physical activity and exercise training confers significant several well-known positive effects for health and CV benefits.1 Therefore, clinicians should continue to promote physical activity while investigating and addressing conventional CV risk factors. However, future longitudinal studies with larger sample sizes are warranted to further clarify the dynamic relationship between exercise, CV risk and CAD in these athletes.
ConclusionsIn the cohort of veteran athletes studied, one fourth presented a high coronary atherosclerotic burden evaluated by CCTA. While a higher volume of exercise combined with high CV risk showed a significant association with coronary atherosclerosis, it tended to be protective in athletes with lower CV risk. These findings underscore the importance of individualized CV risk assessment and exercise prescription in this population, considering the intricate interplay between exercise patterns, CV risk factors, and coronary atherosclerotic burden. Further research is needed to clarify the underlying mechanisms driving these associations and to develop evidence-based strategies for the evaluation of veteran athletes.
Conflicts of interestThe authors have no conflicts of interest to declare.
