
We read the paper by Abreu et al. entitled ‘Coronary arcade: A rare anomaly of the coronary circulation’ with great interest, and we thank them for their interesting report. They asserted that the cause of the chest pain and ECG alterations observed during exercise testing in the case presented may be the result of transient disturbances in coronary blood flow during the test. Furthermore, they state that intercoronary communication (ICC) may be unrelated to ischemia, and that it may even function as a natural bypass, protecting against ischemia.1 Herein, we present our case supporting their idea.
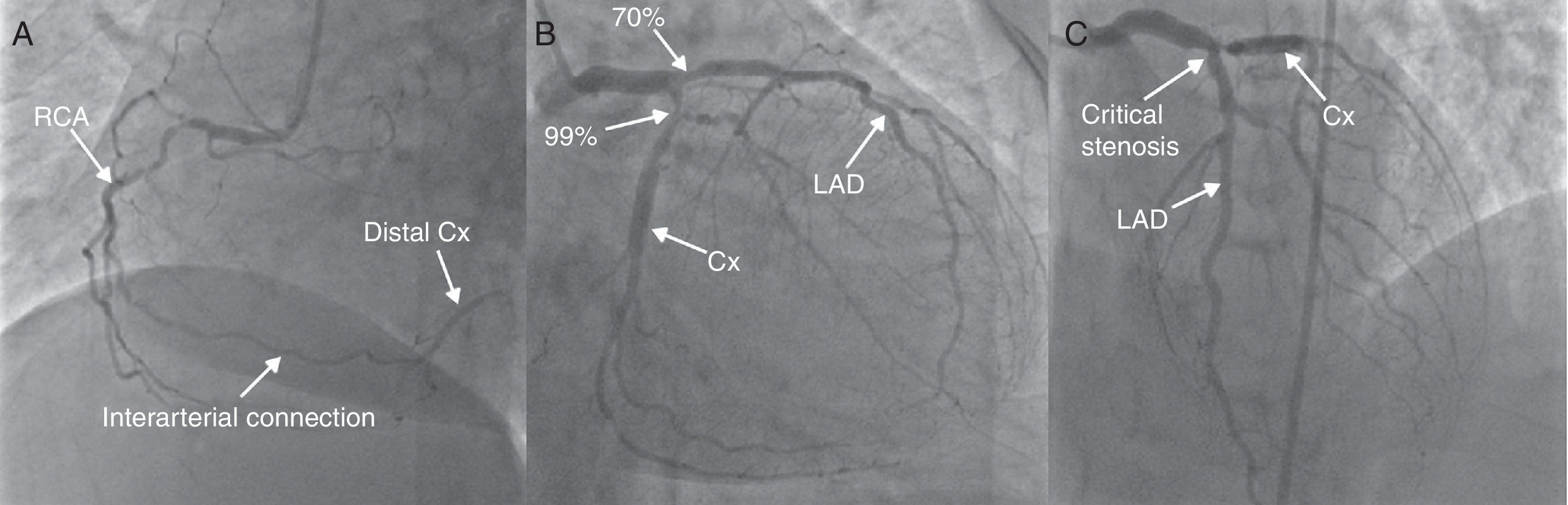
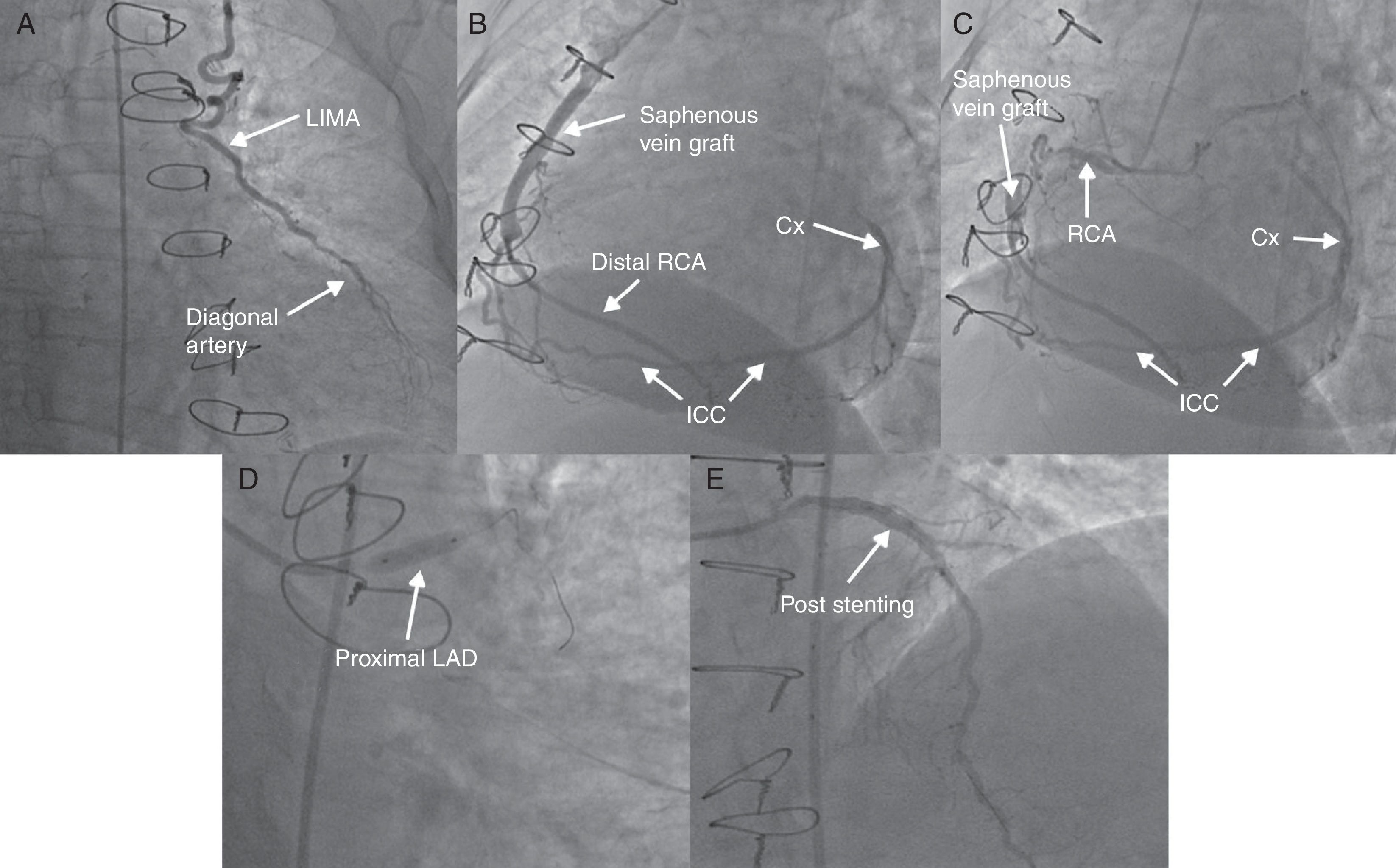
Case reportA 66-year-old woman applied to our clinic with Canadian Cardiovascular Society class III angina pectoris for the last three months. She had type 2 diabetes mellitus, hypertension and hyperlipidemia. She had been treated with triple coronary artery bypass grafting 22 months before (preoperative coronary angiography is shown in Figure 1). Physical examination was normal, while echocardiography demonstrated a hypokinetic anterior wall. Troponin I was positive (0.5 μg/l). Coronary angiography showed critical stenosis in both the proximal segment of the left anterior descending coronary artery (LAD) and the proximal segment of the first diagonal artery, and total occlusion of the proximal left circumflex coronary artery (Cx). The right coronary artery (RCA) had also a critical stenosis in its mid portion. The left internal mammary-diagonal artery graft and the saphenous graft between aorta and RCA were patent (Figure 2A and B), but the aorta-Cx saphenous graft was occluded. The distal Cx was filled by the ICC between the RCA and Cx (Figure 2B and C). We implanted a 3.5 mm×15 mm everolimus-eluting stent (Xience-V) at 16 atm in the proximal LAD (Figure 2D and E). Thus, the ischemic area of the LAD territory was treated by stenting. The other ischemic area had been already protected by the ICC (since birth). The patient was asymptomatic, with no anginal attack or dyspnea, during six months of follow-up.
 the RCA in left oblique projection, (B) the left coronary system in right caudal projection, and (C) the left coronary system in anterior cranial projection. Cx: circumflex artery; LAD: left anterior descending artery; RCA: right coronary artery.")
Preoperative coronary angiography showing (A) the RCA in left oblique projection, (B) the left coronary system in right caudal projection, and (C) the left coronary system in anterior cranial projection. Cx: circumflex artery; LAD: left anterior descending artery; RCA: right coronary artery.
 left internal mammary artery-diagonal artery graft in anterior projection; (B and C) aorta-RCA saphenous vein graft, native RCA and ICC between RCA and Cx in left oblique projection; (D) the stent on anterior caudal projection; and (E) post-stenting LAD in right cranial projection. Cx: circumflex artery; ICC: intercoronary communication; LAD: left anterior descending artery; LIMA: left internal mammary artery; RCA: right coronary artery.")
Postoperative coronary angiography showing (A) left internal mammary artery-diagonal artery graft in anterior projection; (B and C) aorta-RCA saphenous vein graft, native RCA and ICC between RCA and Cx in left oblique projection; (D) the stent on anterior caudal projection; and (E) post-stenting LAD in right cranial projection. Cx: circumflex artery; ICC: intercoronary communication; LAD: left anterior descending artery; LIMA: left internal mammary artery; RCA: right coronary artery.
As stated by Abreu et al. in their article,1 ICC is a very rare coronary anomaly. There are two types of this anomaly. The first is a connection between the Cx and RCA in the posterior atrioventricular groove, while the second is a connection between the LAD and the posterior descending artery in the distal interventricular groove. These connections are congenital and distinct from collateral vessels associated with severe coronary artery disease. Additionally, ICCs are usually larger in diameter and straighter than tortuous collateral vessels.1 Previously reported cases showed that an ICC causes ischemia.2,3 By contrast, a previously reported article revealed an ICC between the RCA and the LAD, providing protection for the totally occluded LAD region.4 Similarly, in our case the ICC also acted as a safety valve against ischemia, supporting the idea put forward by Abreu et al. There was an occluded aorta-Cx saphenous graft in our case. The underlying mechanism of the occluded graft may be sufficient retrograde flow provided by the ICC. If the graft had not been performed, the unidirectional flow through the ICC would have provided enough blood supply. Consequently, the case suggests that if the blood supply to the distal portion of a critical coronary stenosis is being maintained sufficiently to prevent ischemia by an ICC, this critical stenosis may be ignored. Thus, these patients may be protected from prolonged surgery or unnecessary invasive percutaneous procedures.
