
Intercoronary communication or ‘coronary arcade’ is a rare congenital coronary anomaly. We present the case of a 65-year-old man with atypical chest pain for four months. The 12-lead ECG and echocardiogram were normal. Treadmill exercise testing was interrupted at peak exercise due to consecutive salvos of ventricular premature beats, without significant ST-T changes. Coronary angiography showed no significant coronary stenosis, but a connection between the right coronary and circumflex arteries was observed, consistent with coronary arcade. The functional importance of this variant is not clear, but it may cause myocardial ischemia by coronary steal or function as a natural bypass, in which case it may play a protective role in the myocardium if significant atherosclerosis develops.
A comunicação intercoronária ou arcada coronária é uma anomalia rara da circulação coronária de etiologia congénita. Apresentamos o caso de um homem de 65 anos com dor torácica atípica com quatro meses de evolução. O ECG e o ecocardiograma não evidenciavam alterações. Realizou prova de esforço que foi interrompida no pico de esforço máximo por salvas de extrassístoles ventriculares consecutivas, sem alterações ST-T significativas. A coronariografia não revelou estenoses coronárias significativas, contudo, observou-se uma continuidade entre as artérias circunflexa e coronária direita, compatível com arcada coronária. A importância funcional desta anomalia não está esclarecida, porém, poderá causar isquemia miocárdica através de um fenómeno de roubo coronário ou funcionar como um bypass natural e, eventualmente, exercer um papel protetor do miocárdio, caso se desenvolva aterosclerose significativa.
Coronary angiography is commonly used to assess ischemic coronary disease, the result in most cases of atherosclerosis.1 Knowledge of the normal anatomy of the coronary circulation and of congenital anomalies and variants is essential for appropriate treatment of these patients. The prevalence of congenital coronary anomalies in the general population is 1–2%.2,3 Clinical presentation of these anomalies is variable, ranging from clinically silent to life-threatening situations such as myocardial infarction and sudden death.4 Communications between normal coronary arteries are rare congenital anomalies of coronary termination, with an estimated prevalence of 0.05% on diagnostic coronary angiograms.5 This anomaly is a congenital malformation which should not be confused with collateral circulation secondary to obstructive coronary disease.6
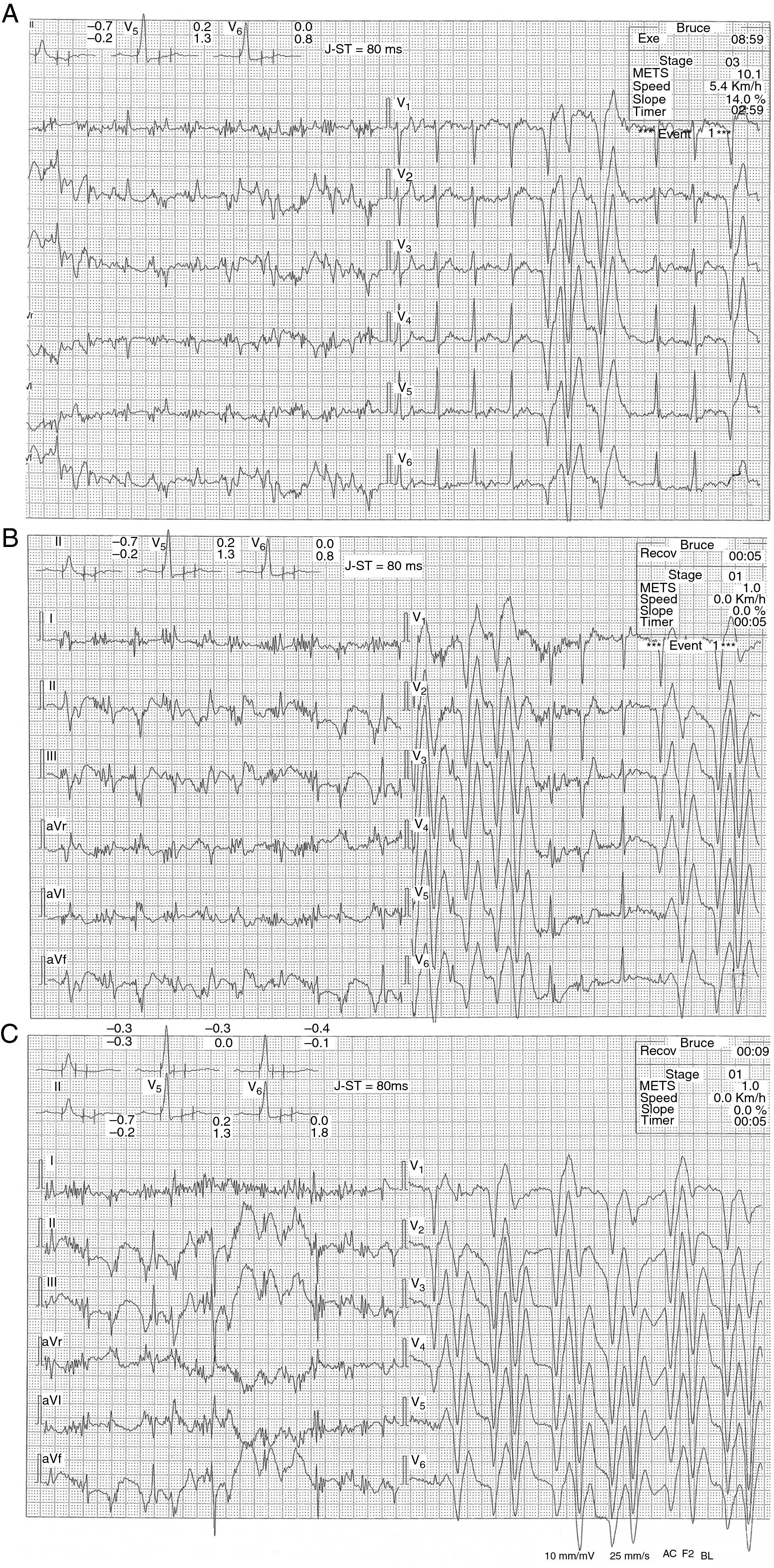
Case reportWe present the case of a 65-year-old man referred for cardiology consultation due to atypical chest pain (dull, unrelated to exertion, lasting a few minutes) for four months. Cardiovascular risk factors included smoking, dyslipidemia and obesity. The physical examination, ECG and echocardiogram were normal. Frequent ventricular ectopy was observed during exercise testing, with consecutive salvos of ventricular premature beats of varied morphology at peak exercise and at the beginning of recovery, without significant ST-T changes (Figure 1). The patient was referred for coronary angiography, which showed coronary artery irregularities but no significant stenosis. Selective angiography of the left coronary artery also revealed the distal portion of the right coronary artery (RCA), due to retrograde filling through an intercoronary connection between the circumflex (Cx) and the RCA (Figure 2). Right coronary angiography showed filling of the Cx and the left anterior descending artery through the same RCA-Cx connection, at the level of the crux (Figure 3). This variant of the coronary circulation is known as intercoronary communication or ‘coronary arcade’. The patient subsequently underwent Holter ECG monitoring, which revealed sinus rhythm, with occasional supraventricular premature beats, 120 isolated polymorphic ventricular premature beats and one pair. He is currently under beta-blocker therapy and is asymptomatic.
, at 5 s into recovery (B), and at 9 s into recovery (C).")
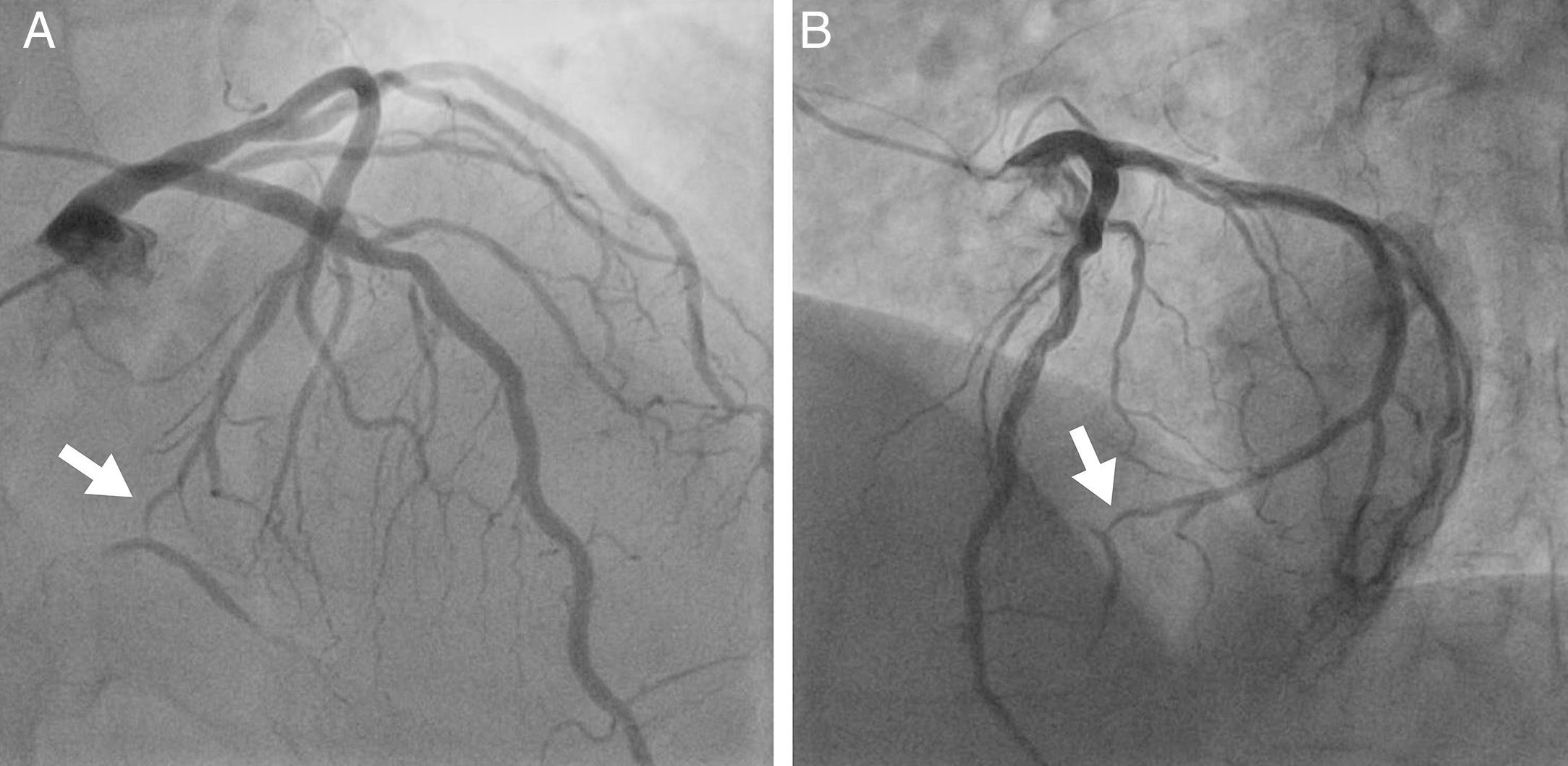
, showing part of the distal segment of the right coronary and posterior descending arteries via an intercoronary connection with the circumflex artery at the level of the crux (arrow).")
Selective angiography of the left coronary artery (A: 10° right anterior oblique, 40° cranial view; B: 45° left anterior oblique, 25° cranial view), showing part of the distal segment of the right coronary and posterior descending arteries via an intercoronary connection with the circumflex artery at the level of the crux (arrow).
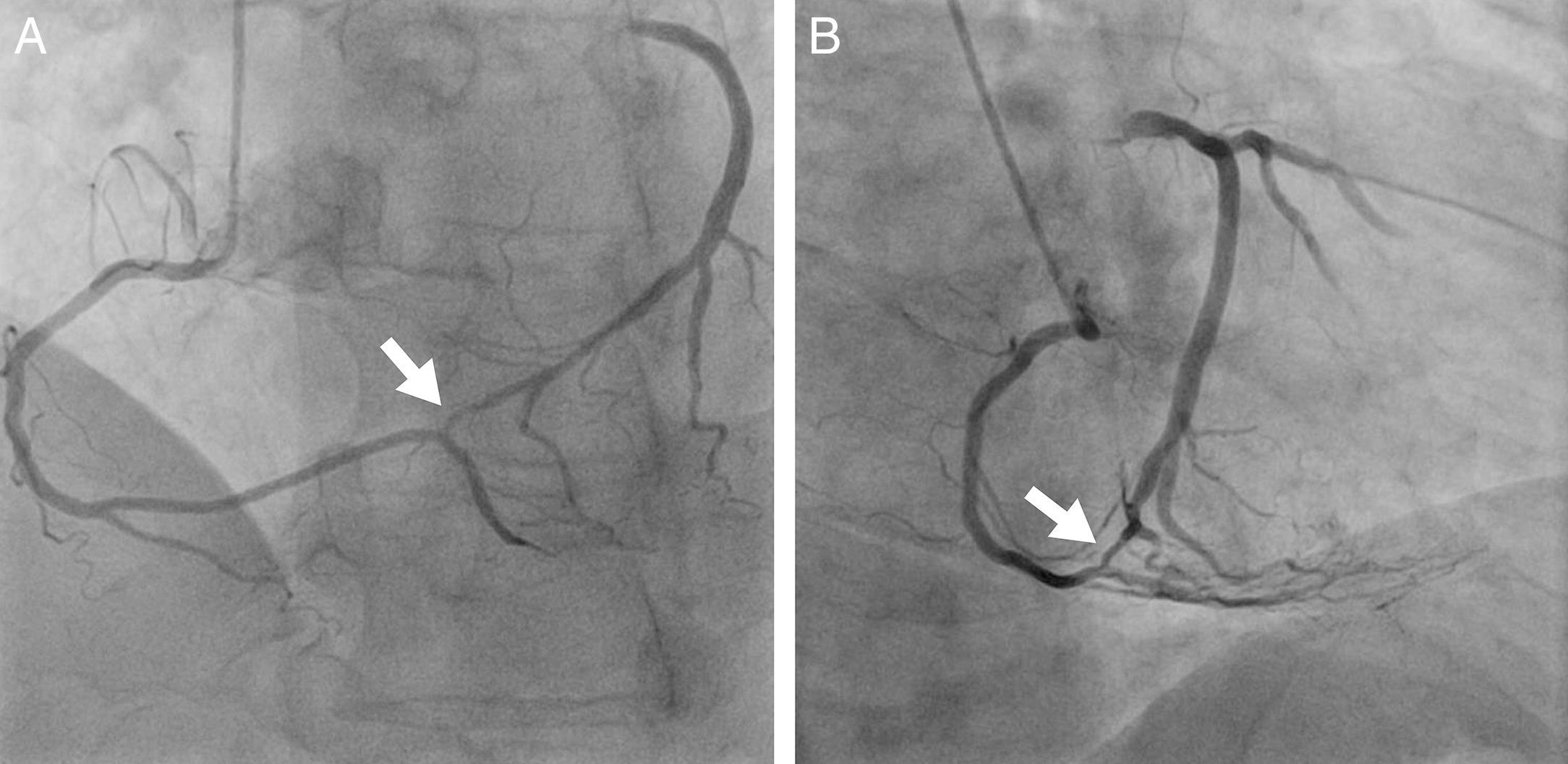
, showing connection between the right coronary and the circumflex arteries (arrow). (A) suggests the presence of coronary arcade and (B) shows the atrioventricular groove, with the atria to the left and the ventricles to the right.")
Right coronary angiography (A: 20° left anterior oblique, 20° cranial view; B: 30° right anterior oblique view), showing connection between the right coronary and the circumflex arteries (arrow). (A) suggests the presence of coronary arcade and (B) shows the atrioventricular groove, with the atria to the left and the ventricles to the right.
Congenital abnormalities in coronary anatomy are termed variants or anomalies. The former are variations of the normal pattern, with relatively common morphological characteristics, and are found in over 1% of the general population, while the latter are uncommon morphological changes found in less than 1% of the population.7 Anomalies and variants of the coronary circulation are divided into four main groups: anomalies of origin, course, termination and intrinsic.8
Intercoronary communication (coronary arcade) is a rare anomaly of termination in which there is communication or open-ended circulation with two-way blood flow between two major coronary arteries. Two types have been described in the literature: communication between the RCA and the Cx in the posterior atrioventricular groove, and communication between the left anterior descending and posterior descending artery in the interventricular groove.9
Unlike collaterals, which are often associated with significant coronary stenosis, coronary arcade is found in angiographically normal coronary arteries. Compared with collaterals, intercoronary arterial connections have a well-defined muscular layer, and are larger in diameter (≥1 mm), extramural and straighter.10
This anomaly of the coronary circulation is assumed to be congenital, due to the persistence of a fetal pattern of coronary circulation. It has been suggested that defective embryonic development allows the existing coronary channel to remain prominent and maintain a large caliber.11
The precise prevalence of this entity is not known; two cases were identified out of 9388 coronary angiograms performed in our hospital in the last ten years (0.02%), a similar figure to that reported in the literature.12
The functional importance of this variant is not clear. It may function as a natural bypass and play a protective role in the myocardium if significant atherosclerosis or atherothrombosis develops.6 On the other hand, it has been suggested that intercoronary communications can cause myocardial ischemia by coronary steal, resulting in inadequate perfusion, particularly when one-way flow is observed on coronary angiography.13 In the case presented, the flow was two-way, since injection of contrast into either the right or left coronary artery led to filling of the contralateral artery.
Interestingly, chest pain was present in all cases reported in the literature, but laboratory evidence of ischemia was almost always inconclusive. We therefore speculate that the pain and ECG alterations observed during exercise testing in our patient were due to transient disturbances in coronary blood flow.6
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Abreu G, Nabais S, Enes V, Marques J, Costa J, Correia A. Arcada coronária – uma anomalia rara da circulação coronária. Rev Port Cardiol. 2014;33:241.e1–241.e5.
