















We present the results of the national cardiac electrophysiology registry of the Portuguese Association of Arrhythmology, Pacing and Electrophysiology (APAPE) and the Portuguese Institute of Cardiac Rhythm for 2021 and 2022.
MethodsData were collected from 26 electrophysiology centers registered with APAPE using an online digital platform. Data collection included information on human and technological resources, electrophysiological studies, ablations performed, atrial fibrillation (AF) ablation, and ventricular tachycardia (VT) ablation procedures.
ResultsIn the 26 centers, 4491 ablations were performed in 2021 and 4968 ablations in 2022. AF ablation was the most frequently performed procedure: 1673 ablations in 2021 and 1994 in 2022, 70% paroxysmal AF, with clinically relevant complications was reported in 1.2–1.5% of the procedures. VT ablation was performed in 294 patients in 2021 (45% with structural disease), and in 331 in 2022 (42% with structural disease). Clinically relevant complications were reported in 2.7–2.4% of the procedures (2021 and 2022, respectively).
ConclusionsIn Portugal, the number of cardiac electrophysiology procedures is on the rise, but it has not reached the levels expected based on European Society of Cardiology data. AF ablation is the most common procedure, accounting for 37% in 2021 and 40% in 2022. VT ablation is still low. Additionally, cardioneuroablation and Brugada syndrome ablation are gaining importance at several Portuguese centers.
Os autores apresentam os resultados do registo nacional de eletrofisiologia cardíaca da Associação Portuguesa de Arritmologia, Pacing e Eletrofisiologia (APAPE) e do Instituto Português do Ritmo Cardíaco (IPRC) relativos a 2021 e 2022.
MétodosForam recolhidos dados dos 26 Centros de Eletrofisiologia registados na APAPE através de uma plataforma digital, sobre recursos humanos e tecnológicos, estudos eletrofisiológicos e ablações realizados, procedimentos de ablação de fibrilação auricular (FA) e de taquicardia ventricular (TV).
ResultadosNos 26 centros de eletrofisiologia, foram realizadas 4491 ablações em 2021 e 4968 ablações em 2022. A ablação de FA foi o procedimento mais realizado: 1673 ablações em 2021 e 1994 ablações em 2022, 70% dos casos de FA paroxística. Foram relatadas complicações clinicamente relevantes em 1,2-1,5% dos procedimentos. A ablação de TV foi realizada em 294 doentes em 2021 (45% com doença estrutural) e em 331 em 2022 (42% com doença estrutural). Foram relatadas complicações clinicamente relevantes em 2,7-2,4% dos procedimentos (2021 e 2022, respetivamente).
ConclusõesA intervenção em Eletrofisiologia Cardíaca mantém um crescimento sustentado em Portugal, embora ainda aquém do expectável, tendo em conta os dados da Sociedade Europeia de Cardiologia. A ablação mais frequente é a da FA (37% em 2021 e 40%em 2022). A ablação da TV está subrepresentada. Os procedimentos de cardioneuroablação e ablação de Síndrome de Brugada começam a ter expressividade nos centros portugueses.

The National Registry of Cardiac Electrophysiology of the Portuguese Association of Arrhythmology, Pacing and Electrophysiology (APAPE) and the Portuguese Institute of Cardiac Rhythm (IPRC) is an observational registry that includes public and private centers that perform electrophysiological (EP) studies and ablations. It assesses the evolution of Portuguese electrophysiology since 1991.1–13 This register translates the human and technological resources of each center, as well as its casuistry, allowing us to analyze its progression over the years.
Data from this registry is also presented in documents from the European Society of Cardiology (ESC) and in the European Heart Rhythm Association (EHRA) White Book.14–16
ObjectivesTo present the results of the national registries for 2021 and 2022, discuss Portuguese electrophysiology data and compare them with official data from different European countries.
MethodsData were collected from all electrophysiology centers registered at APAPE, including a total of 18 public centers and eight private centers. The data were collected and entered into an online digital platform (Cardio Forms) by the coordinator of each center. The data included:
- (1)
human and technological resources,
- (2)
characterization of the EP studies performed, both diagnostic and ablation,
- (3)
characterization of atrial fibrillation (AF) ablation procedures (gender, age, AF classification, ablation technique and complications), and
- (4)
characterization of ventricular tachycardia (VT) ablation procedures (gender, age, etiology, and complications).
All the centers completed the survey. In 2021–2022, there were 26 electrophysiology centers in operation. Of these, 18 were in public hospitals (69%) and eight were in private health institutions (31%). Most of the centers are located in the metropolitan areas of Lisbon and Porto (see Figure 1).

The mean and median number of working hours per week in laboratories were 21 hours and 15 hours, respectively, with a range of 2–60 hours. Only two centers provide urgent/emergent treatments 24/7.
Out of 26 centers, only 12 (46%) have a dedicated room for conducting EP procedures. All centers were equipped with polygraphs, with seven centers having two polygraphs. Only two centers did not have a three-dimensional (3D) electroanatomical mapping system, while 16 centers had at least two of these systems.
With regard to medical human resources, there were 41 electrophysiologists active in 2021–2022. Most centers have 2–3 nurses in their team and one does not have an allocated nurse (Figure 2). There are three centers with nine allied health professionals (cardiac physiologists) in their teams, and two centers that do not have any (Figure 3).
Characterization of electrophysiological procedures
Over the years, there has been a significant increase in the number of EP studies, both diagnostic and involving ablation. However, there was a decrease during the COVID-19 pandemic (Figures 4 and 5). In 2021, there was an increase compared to the pre-pandemic period, with a total of 5141 procedures – of which 650 were diagnostic studies and 4491 were ablations. In 2022, there were 5767 EP studies, which included 802 diagnostic studies and 4968 ablations (Figures 4 and 5).

.")
Regarding the arrhythmias treated via ablation, the most represented were AF, followed by typical atrial flutter and atrioventricular reentry tachycardia (slow pathway ablation) (Figure 6).
. AF: atrial fibrillation; AFL: atrial flutter; AT: atrial tachycardia; AV node: atrioventricular node ablation; AVNRT: atrioventricular reentry tachycardia; PVCs: premature ventricular contractions; VT: ventricular tachycardia.")
Number of ablations according to the arrhythmia diagnosis (2018–2022). AF: atrial fibrillation; AFL: atrial flutter; AT: atrial tachycardia; AV node: atrioventricular node ablation; AVNRT: atrioventricular reentry tachycardia; PVCs: premature ventricular contractions; VT: ventricular tachycardia.
Figures 7 and 8 illustrate the distribution of the EP procedures (diagnostic and ablation) for each center.
 by center (2021).")
 by center (2022).")
The number of centers performing over 300 ablations was six in 2021 and seven in 2022, while six and seven centers performed l<50 ablations in 2021 and 2022, respectively.
The Portuguese position within ESC Centers, according to the 2021 cardiovascular disease statistics is shown in Figure 9.
Atrial fibrillation ablation.")
A total of 1673 AF ablations procedures in 2021 and 1994 in 2022 were performed, in 24 centers, with the highest number of ablations per year at a single center being 373. Most centers performed <50 ablations per year, while a minority conducted >200 ablations annually (see Figure 10).
.")
Regarding the distribution by gender, 62–64% (2021–2022) of the patients were male, with age distribution shown in Figure 11.
.")
According to the AF classification, approximately 70% were paroxysmal, 22% were persistent, and 4–6% were long-standing persistent, showing a relatively stable pattern in recent years (Figure 12).
 ablations, according to type of AF (2018–2022).")
The data indicate that around 15% of the procedures were AF reinterventions (redo cases). In 2021, point-by-point radiofrequency ablation, guided by 3D electroanatomical mapping, was the most frequently used technique, accounting for 60% of cases. This percentage decreased slightly to 53% in 2022. Cryoballoon ablation saw a significant increase and was utilized in 26% of cases in 2021 and 38% in 2022 (Figure 13).
. PVAC: pulmonary veins ablation catheter.")
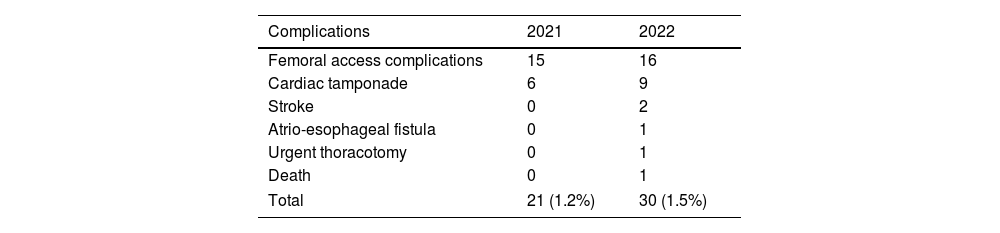
Table 1 represents complications associated with AF ablation. The most frequent were those related to vascular access, followed by cardiac tamponade.
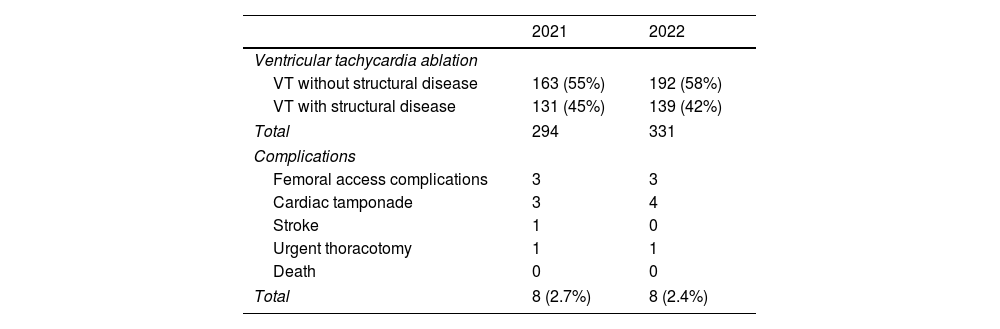
Ventricular tachycardia ablationTable 2 shows the number of VT ablations performed in 2021–2022 and the percentage of underlying structural disease.
Ventricular tachycardia ablations and acute complications associated with ablation.
| 2021 | 2022 | |
|---|---|---|
| Ventricular tachycardia ablation | ||
| VT without structural disease | 163 (55%) | 192 (58%) |
| VT with structural disease | 131 (45%) | 139 (42%) |
| Total | 294 | 331 |
| Complications | ||
| Femoral access complications | 3 | 3 |
| Cardiac tamponade | 3 | 4 |
| Stroke | 1 | 0 |
| Urgent thoracotomy | 1 | 1 |
| Death | 0 | 0 |
| Total | 8 (2.7%) | 8 (2.4%) |
The complications of VT ablation are shown in Table 2. Regarding VT ablation in patients with structural heart disease, most centers performed <10 ablations per year, while the three centers that performed >20 procedures were responsible for 57% of all VT ablations. Figure 14 shows the casuistry of structural VT ablation according to the center.
Discussion
The National Electrophysiology Registry highlights a sustained increase in the number of EP studies, specifically ablations. This reflects the implementation and optimization of resources for differentiated treatments in our patient population.
Despite this, when compared to other European countries with a high number and high volume of centers, we realize that there is still room for improvement. According to a recent document by the ESC on the 2021 cardiovascular disease statistics, an average of 372.3 (ranging from 318.2 to 518.8) ablation procedures per million inhabitants of ESC member countries were performed for the treatment of heart rhythm disorders.17 Rates ranged from <25 procedures per million people in Bosnia and Herzegovina, Egypt, Kyrgyzstan, and Uzbekistan, to >700 procedures per million people in Belgium, Czech Republic, France, Germany, Iceland, and Switzerland; Portugal reported 395.3 ablations per million inhabitants.
The distribution of EP doctors, nurses, and cardiac physiologists in the present registry is markedly heterogeneous with regard to the allocation of resources.
The specificity and technical innovation of electrophysiology require continuous training and dedication, which means it is extremely important to maintain training programs and include dedicated nurses and cardiopulmonary technicians in the EP teams. The number of electrophysiologists is low compared to the number of active centers; this is a national phenomenon most likely related to the fact that most evolution over time in EP procedures reveals that there has been a significant increase in AF and VT ablations. In 2021–2022, there was also some relevance in cardioneuroablation and Brugada syndrome ablation.
Despite an increase in the number of VT ablations in patients with structural heart disease, this figure does not fully represent the population of patients requiring interventional treatment for VT. Several constraints could explain this, including the absence of an organized network for referral centers and logistical limitations in high-volume centers. Severely ill patients experiencing an arrhythmic storm and admitted to emergency care justify the need for a program that provides a pathway strategy, allowing for a quick approach and treatment in centers with higher expertise. In a survey conducted by the European Heart Rhythm Association in 88 centers from 12 countries performing EP studies, most centers performed <50 ablation procedures per year. There were different ablation strategies and endpoints utilized, highlighting the need for standardization in this interventional therapy.18
Cardioneuroablation gained some expressiveness in the national caseload. It has been performed in five public and three private centers, all of which are hospitals where pulmonary vein isolation procedures are carried out. Although the technique has not yet been included in the ESC recommendations, it has been shown to be useful in treating cardioinhibitory reflex syncope, especially in a younger population where there are clear benefits, despite the guidelines not specifying its use.19–21
Epicardial ablation in Brugada syndrome was performed in high-volume centers with experience in epicardial access and mapping. However, since it is a specific procedure for a very select group of patients, it is unlikely we will see a significant increase in the number of these procedures performed in the coming years.
Due to its high prevalence in the population, AF ablation plays an important role in electrophysiology laboratories. Multiple recent studies have shown that it is safer and yields better outcomes than antiarrhythmic drugs. As a result, there is expected to be a growing impact, and EP centers will need to organize themselves to optimize the interventional treatment of this common arrhythmia. The guidelines from scientific societies recommend that a minimum of 50 AF ablations be performed during an EP fellowship. They emphasize the importance of performing several AF ablation procedures each year to maintain expertise and ensure safety and success.22 Our data indicate that some centers have a low number of AF procedures annually. Despite the low rate of acute ablation complications, it is important to monitor AF recurrences and outcomes in future surveys. We should also work on developing local teams to increase activity and maintain safety and effectiveness.
We observed an increase in the referral of patients with persistent and long-standing persistent AF and elderly groups. In our data, around 30% of cases involved non-paroxysmal AF; most patients were between 60 and 69 years old, 24% were between 70 and 79 years old, and 12 patients were >80 years old.
The number of cryoballoon ablations has significantly increased, which is likely due to its “single-shot” technique, making it less time-consuming compared to radiofrequency ablation. Several studies have shown similar results between the two methods.23,24 Cryoablation procedures were performed in nine public centers and six private centers; the increase in numbers was mainly attributed to high-volume centers. The introduction of pulsed field ablation may, however, lead to a decline in the use of cryoablation.
Complications associated with AF ablation occurred in 1.2–1.5% of the procedures, a lower percentage compared to that found in the literature. The most frequent complication was related to vascular access, similarly to the findings observed in VT ablation.22 With the growing evidence of the added value of ultrasound-guided vascular puncture in terms of complications and fluoroscopy reduction, its use in daily practice is certainly expected, with a potential reduction in vascular complications.25
LimitationsOne limitation of this registry is that the survey is based on voluntary participation without independent monitoring. All data were entered by the EP center coordination, and not all centers provided specific diagnoses for the total number of ablations. Additionally, there was no information about the number of ablations compared to the number of patients, as some patients may receive more than one arrhythmic substrate ablation in the same procedure. Another limitation is the lack of data on the success rates of ablations performed during the period of EP activity under analysis. Future registries should address these issues to improve the quality of national data on EP diagnosis and ablations.
ConclusionsThe field of electrophysiology is steadily growing in Portugal, both in public and private healthcare facilities. However, the rate of ablations per million inhabitants still falls below the data published by the ESC. AF is the most common arrhythmia treated with ablation, reflecting the aging population and the proven clinical benefits of this treatment. VT ablation appears to be underrepresented and is mostly conducted in high-volume centers, highlighting the need for a referral networking program. Procedures such as cardioneuroablation and Brugada syndrome ablation are gaining prominence, particularly at high-volume centers.
Ethical statementThe authors declare that no experiments were performed on humans or animals for this study. The authors declare that they have followed the protocols of their work center on the publication of patient data. The authors declare that no patient data appear in this article.
Declaration of generative AI and AI-assisted technologies in the writing processThe authors declare that they did not use artificial intelligence to prepare this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors are grateful for the important contributions of the following specialists who provided data for the registry: Dr. Francisco Madeira (Hospital Fernando Fonseca), Dr. Francisco Morgado (Hospital dos Lusíadas), Dr. Hipólito Reis (Hospital de Santo António – CHUP), Dr. João de Sousa (Hospital de Santa Maria – CHULN; Hospital SAMS), Dr. João Primo (Centro Hospitalar Vila Nova de Gaia; Hospital da Luz – Arrábida), Professor Leonor Parreira (Hospital de São Bernardo – CH Setúbal), Dr. Luís Adão (Hospital de São João – CHUSJ), Dr. Luís Brandão (Hospital Garcia de Orta; Hospital CUF Infante Santo), Dr. Luís Elvas (Hospitais da Universidade de Coimbra – CHUC); Dr. Luís Santos (Hospital de São Teotónio – CH Tondela-Viseu); Professor Mário Oliveira (Hospital de Santa Marta – CHLC; Hospital CUF Infante Santo; Hospital CUF Porto), Dr. Nuno Santos (Hospital Dr. Nélio Mendonça – HC Funchal), Professor Pedro Adragão (Hospital de Santa Cruz – CHLO; Hospital da Luz – Lisbon), Dr. Pedro Silva Cunha (Hospital da Cruz Vermelha), Dr. Renato Margato (Hospital São Pedro de Vila Real – CHTAD), Dr. Rui Candeias (Hospital de Faro – CHUA), Dr. Sónia Magalhães (Hospital de Braga), and Dr. Víctor Sanfins (Hospital da Senhora da Oliveira – Guimarães).
