

Ebstein's anomaly (EA) is a rare congenital malformation of the tricuspid valve, often associated with other cardiac malformations, especially atrial septal defect, which is present in 80–90% of patients and predisposes to paradoxical embolization. We describe the case of a 47-year-old male, a drug abuser, with a known but not investigated cardiac murmur. He presented to the emergency department with worsening exertional dyspnea and fatigue associated with recent recurrent transient ischemic attacks. On brain computed tomography there were multiple non-recent ischemic infarctions. Transthoracic echocardiography showed EA with severely dilated right cardiac chambers, right systolic dysfunction and severe tricuspid regurgitation. Contrast and transesophageal echocardiography revealed a patent foramen ovale with right-to-left shunt. After exclusion of other potential causes of the neurologic events, they were assumed to be the consequence of paradoxical embolism.
A anomalia de Ebstein é uma malformação congénita rara da válvula tricúspide, geralmente associada a outras malformações congénitas, particularmente os defeitos do septo auricular, que podem estar presentes em cerca de 80% a 90% dos doentes e favorecer a embolia paradoxal. Descrevemos o caso de um homem de 47 anos de idade, toxicodependente, com história de sopro cardíaco conhecido de longa data, mas não estudado. Recorreu ao Serviço de Urgência por dispneia e fadiga de esforço com agravamento progressivo associados a eventos recorrentes de acidentes isquémicos transitórios. A TC cerebral evidenciou múltiplas lesões isquémicas sequelares não recentes. A ecocardiografia transtorácica revelou a presença de anomalia de Ebstein com dilatação severa das cavidades direitas, disfunção ventricular direita e regurgitação tricúspide severa. O ecocardiograma com contraste e transesofágico permitiram evidenciar a coexistência de foramen oval patente com shunt direita-esquerda. Foram excluídas outras possíveis causas explicativas para o quadro neurológico, que se assumiu na dependência de embolismo paradoxal.
Ebstein's anomaly is a rare congenital tricuspid valve malformation which causes ‘atrialization’ of the right ventricle. It represents about 0.5% of congenital heart defects and only 5% of cases survive beyond the age of 50.1 It is characterized by clinical highly variable clinical manifestations and outcome, which depend on the diversity and severity of the underlying anatomic changes.2 It is usually associated with other congenital defects, particularly atrial septal defect, which may be present in 80–90% of patients and predispose to paradoxical embolism.3,4
Case reportThe authors describe the case of a 47-year-old male, a drug abuser (cocaine, heroin and hashish), on a methadone program for one year, a smoker and alcohol abuser and with a cardiac murmur detected several years previously, not investigated and without medical surveillance. He was admitted to the emergency department with exertional dyspnea and worsening fatigue and short (about 30 minutes) self-limiting recurrent events of right hemiparesis and hemihypoesthesia. On physical examination, he was hemodynamically stable (blood pressure 136/75 mmHg; heart rate 68 bpm), eupneic at rest, with jugular swelling at 30° and a holosystolic murmur on the left sternal border, but no carotid murmur or neurologic deficit.
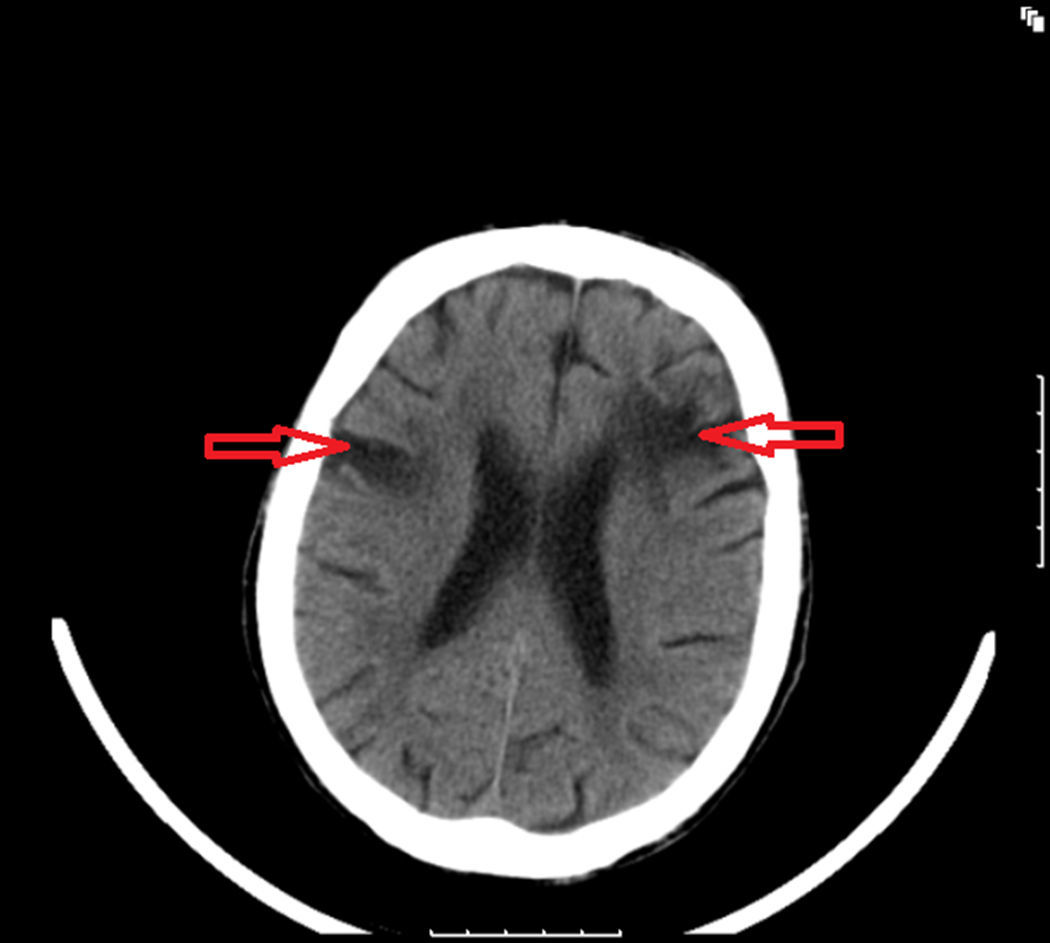
Laboratory tests, including coagulation study, were normal. Brain cardiac tomography showed ischemic lesions with multiple non-recent ischemic sequelae (Figure 1) and no changes on cervical Doppler ultrasound. The electrocardiogram showed sinus rhythm (heart rate 61 bpm), first-degree atrioventricular block, right atrial abnormality, poor R-wave progression in the anterior wall and Q waves in the inferior leads. The chest X-ray documented cardiomegaly due to enlargement of the right cardiac chambers (Figure 2).
.")
 and left convexity suggests dilatation of the right ventricular outflow tract.")
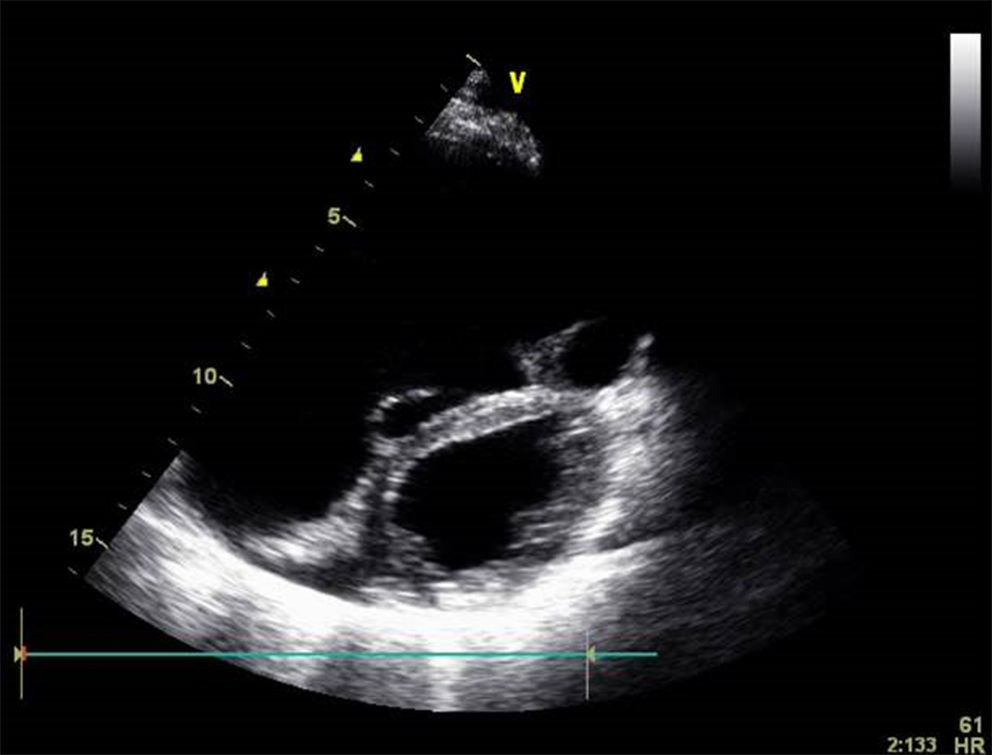
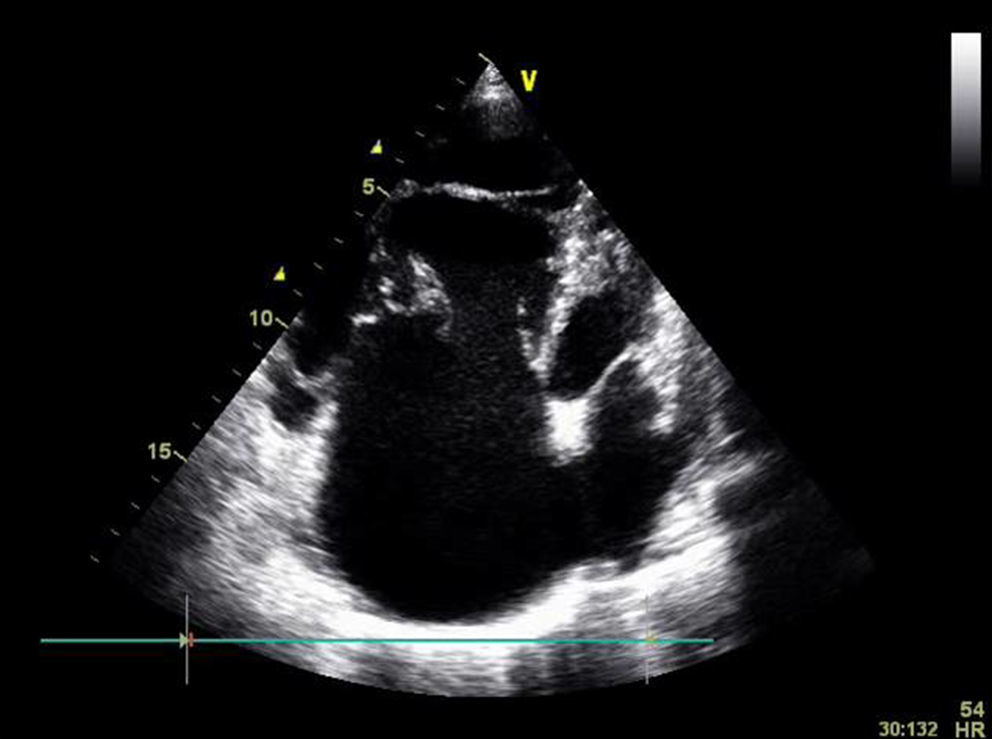
The transthoracic echocardiogram showed dilated right heart chambers (Figure 3), abnormal tricuspid valve with myxomatous asymmetric appearance and tethering of the tricuspid valve septal leaflet (possible infectious or congenital etiology – endocarditis or possible sequelae of cleft leaflet) with consequent severe tricuspid regurgitation due to poor leaflet coaptation (Figure 4), pulmonary systolic arterial pressure estimated at 44 mmHg, apparently preserved global left ventricular systolic function, and no images suggestive of vegetations or other intracavitary masses. Administration of intravenous contrast (agitated saline) revealed a right-to-left shunt. Transesophageal echocardiography subsequently confirmed that the shunt was due to a patent foramen ovale.

.")
In view of the patient's history of multiple recurrent transient ischemic attacks, likely due to cardioembolic etiology (paradoxical embolism), it was decided to start anticoagulation therapy. After cardiac catheterization, which excluded significant coronary artery disease, the patient underwent surgical correction (tricuspid valve repair with ring placement, right ventricular plasty and patent foramen ovale closure), without complications and with subsequent clinical improvement.
Discussion and ConclusionEA in adulthood is often a benign and stable disease, especially in asymptomatic patients.3 However, clinical manifestations depend on the structural and functional alterations in the right cardiac chambers as well as in tricuspid valve morphology, and are more severe the greater the displacement of leaflet insertion.5 The clinical presentation can also be affected by other congenital malformations which are often associated, the most frequent of which is atrial septal defect.2–4 In the presence of septal defect, the increased right atrial pressure induced by the hemodynamic and functional changes resulting from EA cause reversed shunting (right-to-left), which is an anatomical substrate for paradoxical embolism that can lead to in stroke,4,5 as demonstrated in this case.
The unusual nature of the case presented and its successful outcome prompted publication in this report.
Conflicts of interestThe authors have no conflicts of interest to declare.
