

An 82-year-old woman with a history of hypertension and degenerative arthritis of multiple joints, ‘bamboo spine’, bilateral total knee and hip replacements (Figure 1) and blue-gray ocular deposits on both conjunctivae (Figure 1B), presented with New York Heart Association class III symptoms of heart failure lasting for six months. Transthoracic echocardiography revealed severe aortic stenosis (AS) with peak and mean aortic valve gradients of 105 and 61 mmHg, respectively, a valve area of 0.46 cm2, left ventricular hypertrophy and preserved systolic function. The coronary angiogram revealed non-significant stenosis in the left anterior descending coronary artery. Computed tomography angiography showed a porcelain aorta (Figure 2). Transcatheter aortic valve replacement (TAVR) with a 23-mm Edwards SAPIEN 3 valve was performed successfully.
 and blue-gray ocular deposits on both conjunctivae (B).")
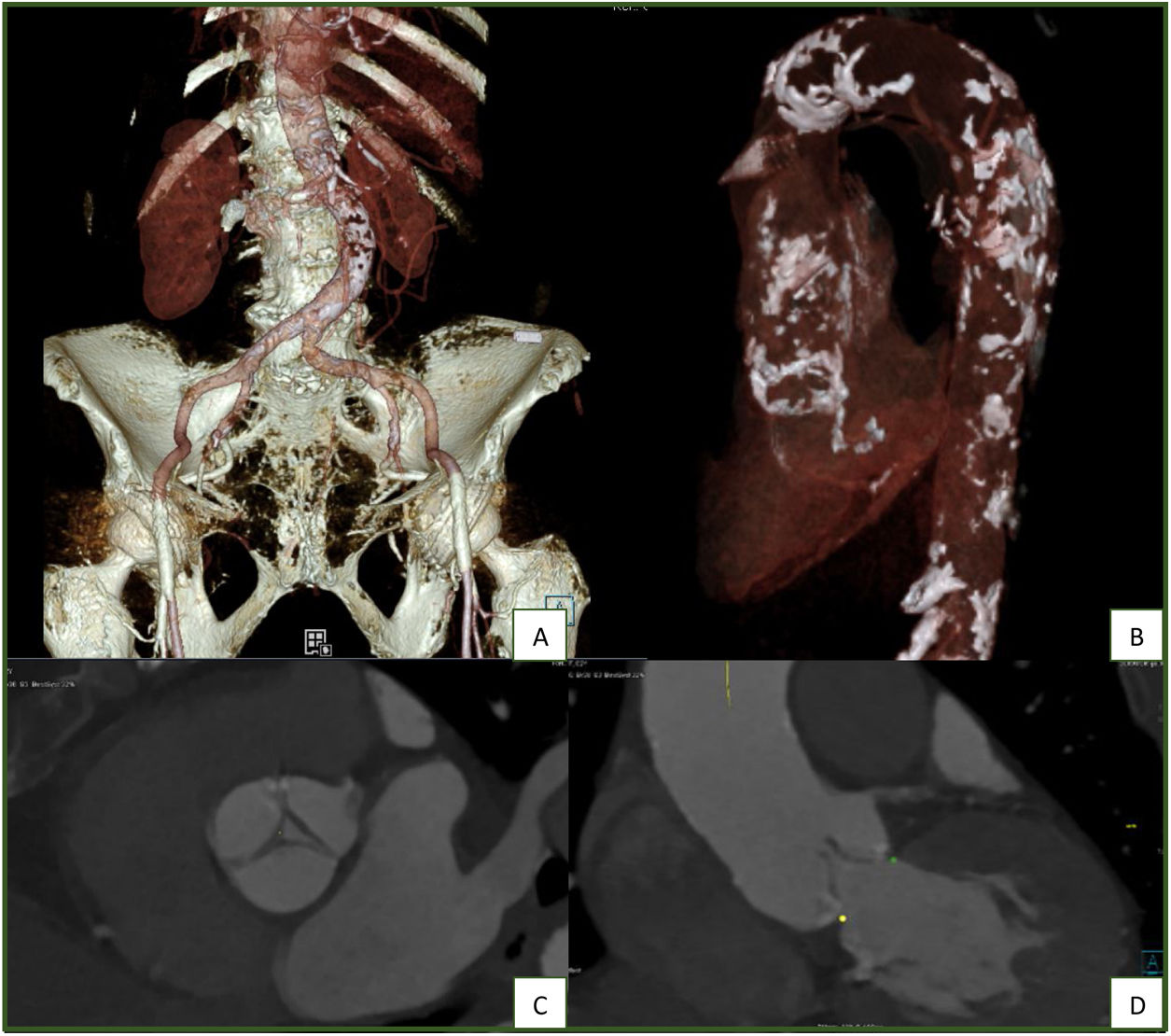
 reconstruction of the abdominal aorta and iliofemoral arteries, the latter without significant calcification or stenosis (A); left anterior oblique VRT reconstruction of the thoracic aorta, disclosing extensive, multifocal calcified plaques (porcelain aorta) (B); short-axis (C) and coronal (D) reconstructions of the aortic valve at 20% of the RR interval, disclosing restricted systolic leaflet motion and mild commissural calcification.")
Volume rendering technique (VRT) reconstruction of the abdominal aorta and iliofemoral arteries, the latter without significant calcification or stenosis (A); left anterior oblique VRT reconstruction of the thoracic aorta, disclosing extensive, multifocal calcified plaques (porcelain aorta) (B); short-axis (C) and coronal (D) reconstructions of the aortic valve at 20% of the RR interval, disclosing restricted systolic leaflet motion and mild commissural calcification.
The patient had been diagnosed with alkaptonuria, a rare autosomal recessive genetic disorder of tyrosine metabolism that produces a deficiency of the enzyme homogentisate dioxygenase causing high circulating levels of homogentisic acid (HGA).1 This disease has a worldwide incidence of 1 per 250000 live births and leads to ochronosis, skin pigmentation, degenerative arthropathy and AS.2 Life span is not usually shortened in alkaptonuria, but quality of life is severely affected.
Treatment for alkaptonuria-associated AS has mostly involved surgical aortic valve replacement and there have been few reports of successful TAVR.3 It is unclear whether biological prosthetic valves are exposed to the same process of HGA deposition and calcification, which would affect prosthesis longevity.4
We report a successful TAVR for alkaptonuria-associated AS in a patient deemed inoperable because of extensive calcification of the aortic root.
FundingNone declared.
Conflicts of interestThe authors have no conflicts of interest to declare.
