
A 46-year-old woman had been diagnosed with atrial septal defect (ASD) with bidirectional shunt at the age of five years, when the hemodynamic study showed mild supravalvular aortic stenosis and severe untreatable diffuse stenosis of the peripheral pulmonary arteries.
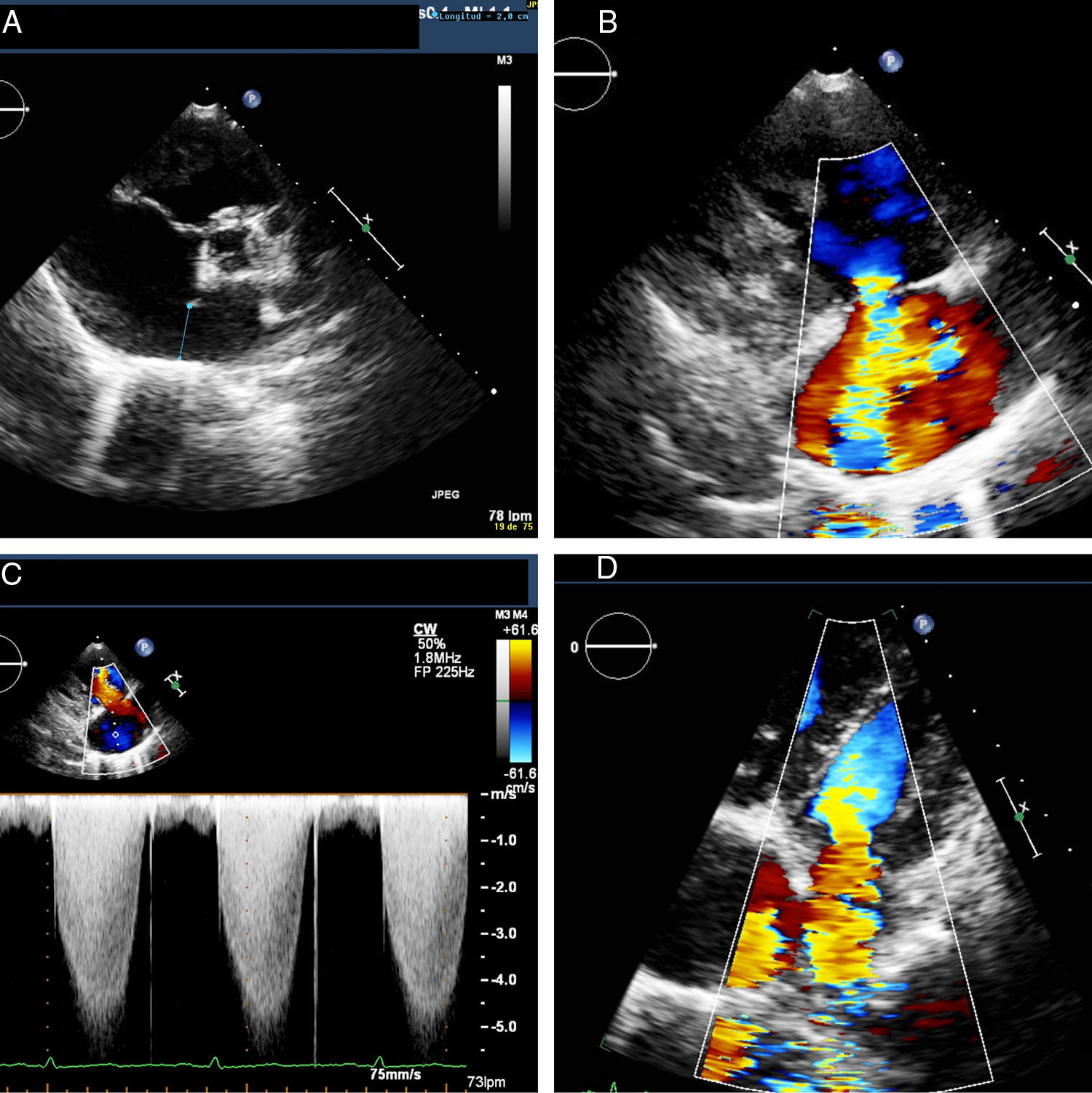
Her situation was reassessed after an episode of atypical chest pain and palpitations with negative ischemia testing. The echocardiogram revealed moderate right ventricular (RV) dilatation with severe hypertrophy and preserved systolic function, a large ostium secundum ASD with predominantly left-to-right bidirectional shunt (Figure 1A), severe tricuspid regurgitation (Figure 1B and C), and moderate mitral regurgitation (Figure 1D) with evidence of severe pulmonary hypertension and dilatation of the pulmonary trunk.
, severe tricuspid regurgitation (B and C) and moderate mitral regurgitation (D).")
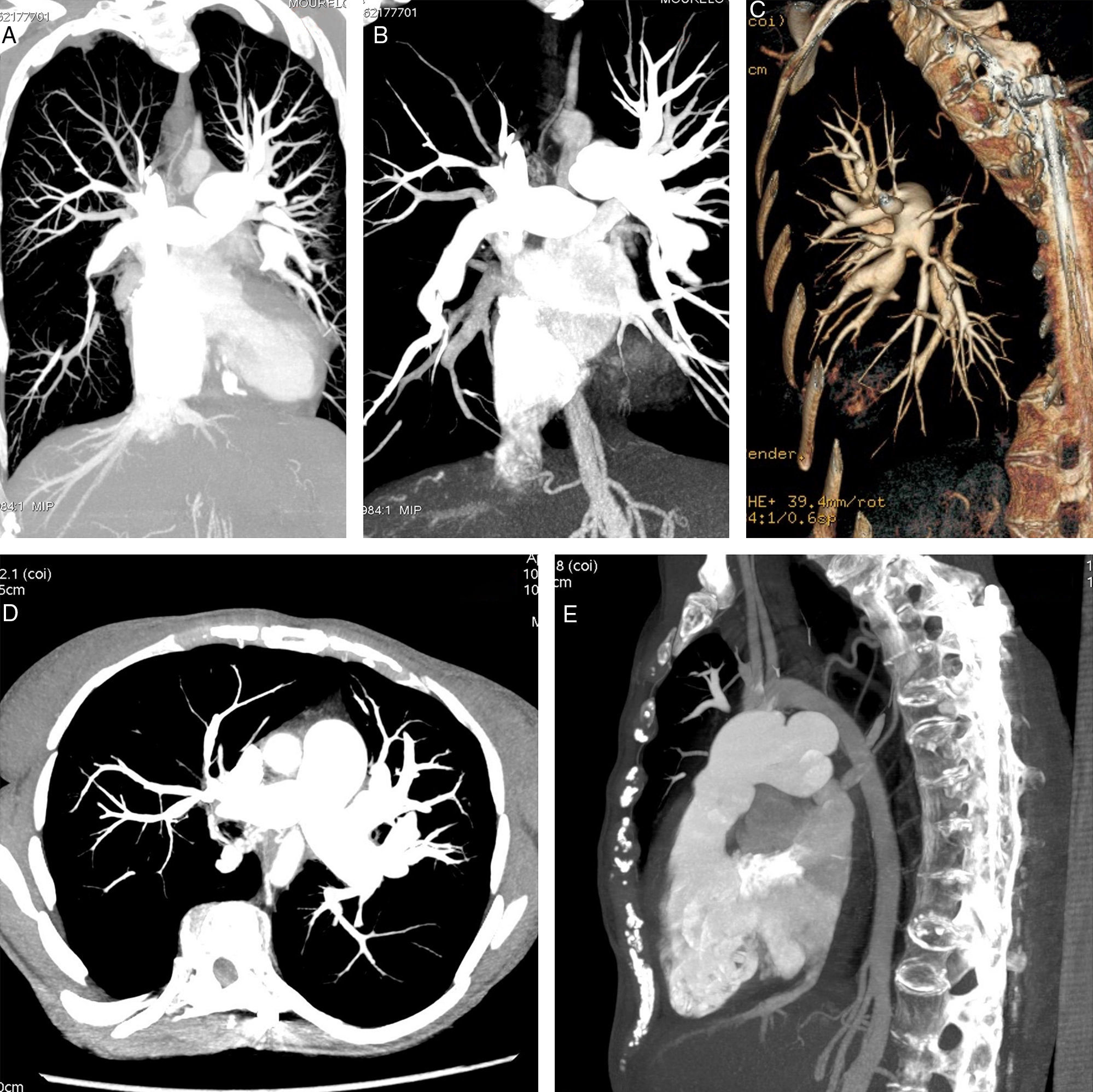
Given this background, she was referred for computed tomography (CT) angiography to assess the pulmonary tree and to examine the therapeutic possibilities. This study confirmed severe stenosis at the origin of most of the lobar pulmonary arteries and diffuse stenosis of the rest (Figure 2A-D) and underdevelopment of the aortic arch (Figure 2E). Given these findings, no type of intervention was performed, opting for clinical follow-up and medical treatment.
, and underdevelopment of the aortic arch (E).")
Segmental pulmonary stenosis is a rare disease of unknown etiology, usually associated with complex congenital heart disease or clinical syndromes such as Williams syndrome. The prognosis is uncertain and is influenced by the degree of involvement, treatment options, and RV function. In cases of severe and multiple stenosis unsuitable for corrective treatment, the occurrence of RV dysfunction is the main prognostic factor, but it is unpredictable, and our patient, now 46 years old, has shown no dysfunction or signs of right heart failure.
The excellent spatial and temporal resolution of CT angiography enables accurate assessment of the anatomy of the pulmonary arterial tree, limited only by the radiation dose and the need for contrast.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Conflicts of interestThe authors have no conflicts of interest to declare.
