
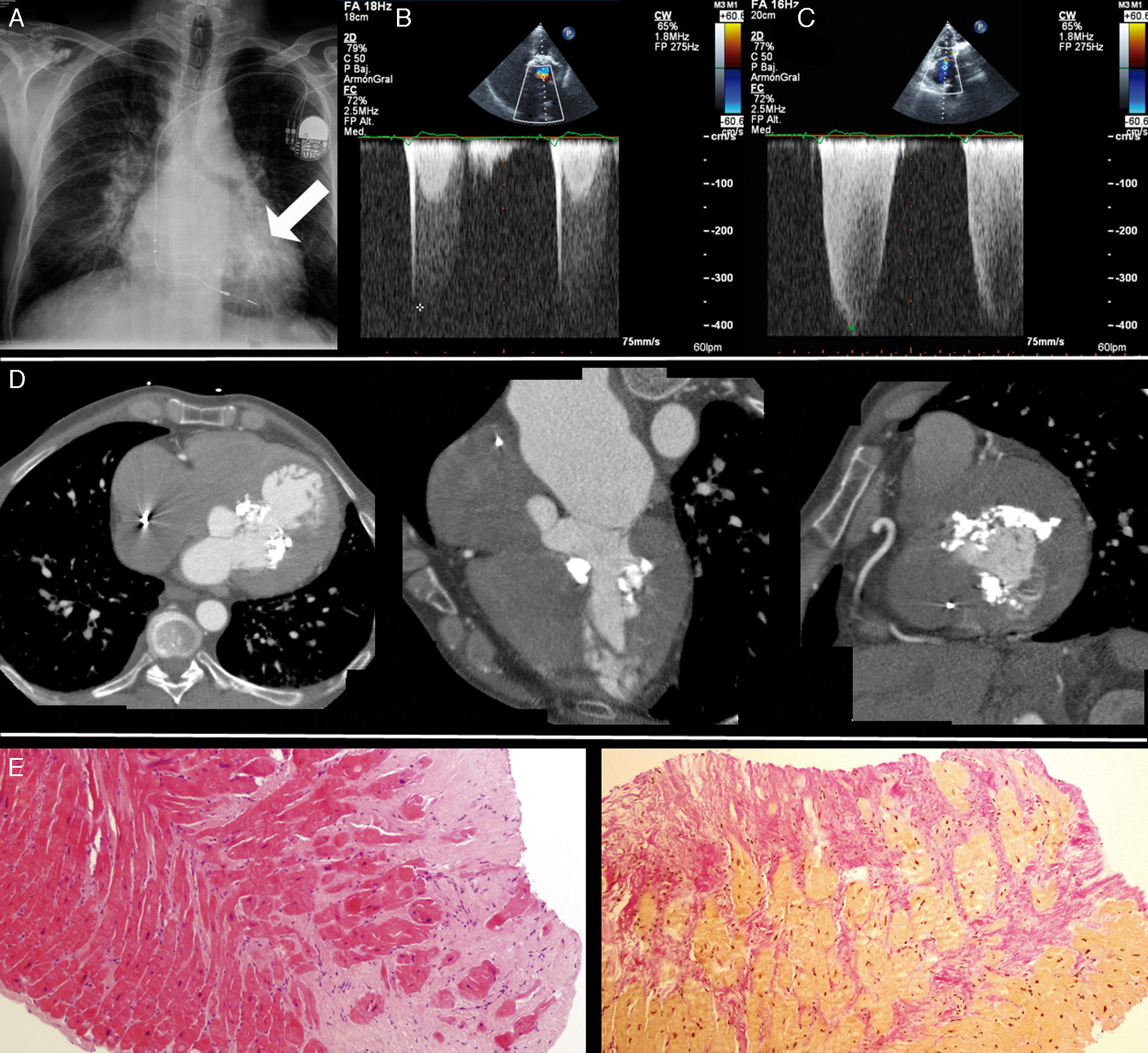
A 40-year-old male with an implanted pacemaker, who had lived in a tropical country for more than 15 years, was admitted because of congestive heart failure. The chest X-ray showed mild cardiomegaly and marked calcification of the left ventricle (Figure 1A, arrow). The transthoracic echocardiogram revealed left ventricular thickening, calcification of the basal segments (Videos 1–3), significant intraventricular gradient (Figure 1B) and severe pulmonary hypertension (Figure 1C). Cardiac computed tomography (CT) confirmed the presence of endomyocardial calcification of the basal anteroseptal and basal inferior left ventricular walls (Figure 1D). Coronary angiography ruled out coronary artery disease and endomyocardial biopsy demonstrated foci of endomyocardial fibrosis (Figure 1E). Treatment with furosemide and spironolactone was started. After the addition of beta-blockers, a decrease in intraventricular gradient (52 mmHg to 30 mmHg) was seen and a significant improvement in symptoms was observed. After three-month follow-up the patient is stable in NYHA class II.
. Panels B and C: Continuous-wave Doppler echocardiographic evaluation showing intraventricular gradient and severe pulmonary hypertension respectively. Panel D: Cardiac-CT showing calcification of the basal anteroseptal and basal inferior left ventricular walls. Panel E: Endomyocardial biopsy depicting normal myocardium surrounded by foci of endomyocardial fibrosis.")
Panel A: Chest X-ray depicting left ventricular calcification (arrow). Panels B and C: Continuous-wave Doppler echocardiographic evaluation showing intraventricular gradient and severe pulmonary hypertension respectively. Panel D: Cardiac-CT showing calcification of the basal anteroseptal and basal inferior left ventricular walls. Panel E: Endomyocardial biopsy depicting normal myocardium surrounded by foci of endomyocardial fibrosis.
Endomyocardial fibrosis is an infrequent disease, more prevalent in tropical countries, that causes progressive restrictive cardiomyopathy leading to congestive heart failure. The presence of endomyocardial calcification in this condition is very rare. Although calcified opacities in the left ventricle may be seen on the chest X-ray, other imaging tests are needed to establish the diagnosis. Given the acoustic shadowing caused by the calcium, echocardiography is technically limited as a diagnostic tool, but it may be useful to evaluate the hemodynamic repercussions of the calcification. Calcium strongly attenuates X-rays, appears bright on CT scans and is readily differentiated from surrounding tissue. Cardiac CT is therefore an accurate technique to evaluate the extent and anatomic distribution of endomyocardial calcification.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
