
The potential anti-inflammatory effect of colchicine has been explored in many conditions, including pericarditis. The Cochrane Collaboration Systematic Review included four randomized controlled trials enrolling 564 patients with acute pericarditis (two studies) or recurrent pericarditis (two studies), followed for a period of 20–24 months. Colchicine was associated with a significant reduction in short-term persistence of chest pain and in long-term risk of recurrence of pericarditis. No significant increase in overall adverse events was observed. Despite the available evidence, the use of colchicine in this context remains strictly off-label.
O potencial anti-inflamatório da colchicina tem vindo a ser avaliado em várias patologias, incluindo a pericardite. A revisão sistemática da Cochrane incluiu quatro ensaios clínicos aleatorizados e controlados, com 564 doentes com pericardite aguda (dois estudos) e pericardite recorrente (dois estudos), seguidos por um período de 20-24 meses. A colchicina esteve associada a uma redução significativa do risco de persistência de dor torácica (curto prazo) e do risco de recidiva de pericardite (longo prazo), sem aumento significativo dos eventos adversos totais. Apesar da evidência disponível, o uso de colchicina neste contexto mantém-se off-label.
What is the impact of colchicine in preventing the recurrence of pericarditis?
ObjectiveTo assess the effects of colchicine as monotherapy or in combination to prevent further recurrences of pericarditis.
Description of reviewThe authors carried out a systematic review of randomized controlled trials (RCTs) assessing the effects of colchicine in patients with idiopathic acute or recurrent pericarditis.1 All interventions with colchicine were included, including those with additional therapy such as non-steroidal anti-inflammatory drugs (NSAIDs) or steroids, and any type of control, whether inactive (placebo) or active (e.g. aspirin, NSAIDs or steroids).
The following databases were searched: Cochrane Central Register of Controlled Trials (CENTRAL, July 2014 issue), MEDLINE (1946 to 2014), EMBASE (1947 to 2014), Conference Proceedings Citation Index-Science on Web of Science (1990 to 2014), and databases of international registries of clinical trials (International Clinical Trials Registry Platform Search Portal, ClinicalTrials.gov, and European Union Clinical Trials Register).
Data were pooled in meta-analyses. Hazard ratios (HR) with 95% confidence intervals (CI) were used to express events such as time until the first recurrence of pericarditis and dichotomous variables were expressed as risk ratios (RR) with 95% CI. In cases of statistical significance the number needed to treat (NNT) was calculated.
ResultsFour trials were included, with follow-up ranging from 20 to 24 months. Two were open-label, with controls receiving the anti-inflammatory therapy recommended for pericarditis, and two were double-blind and placebo-controlled. A total of 564 participants were included (64% with acute and 36% with recurrent pericarditis), most of the latter (>75%) diagnosed with idiopathic pericarditis.
All participants received aspirin at cumulative doses of 2.4–3.2 g daily for a week, gradually tapered down over a period of 3–4 weeks. In two trials, ibuprofen 600 mg in three daily doses was additionally offered as an alternative to aspirin. People who had contraindications to aspirin received steroids.
Colchicine was administered orally, and in three trials was given at a loading dose of 1 mg every 12 hours for the first day. A maintenance dose of 0.5 mg twice daily (once daily for those weighing <70 kg) was then continued for three months in patients with acute pericarditis and six months in those with recurrent pericarditis.
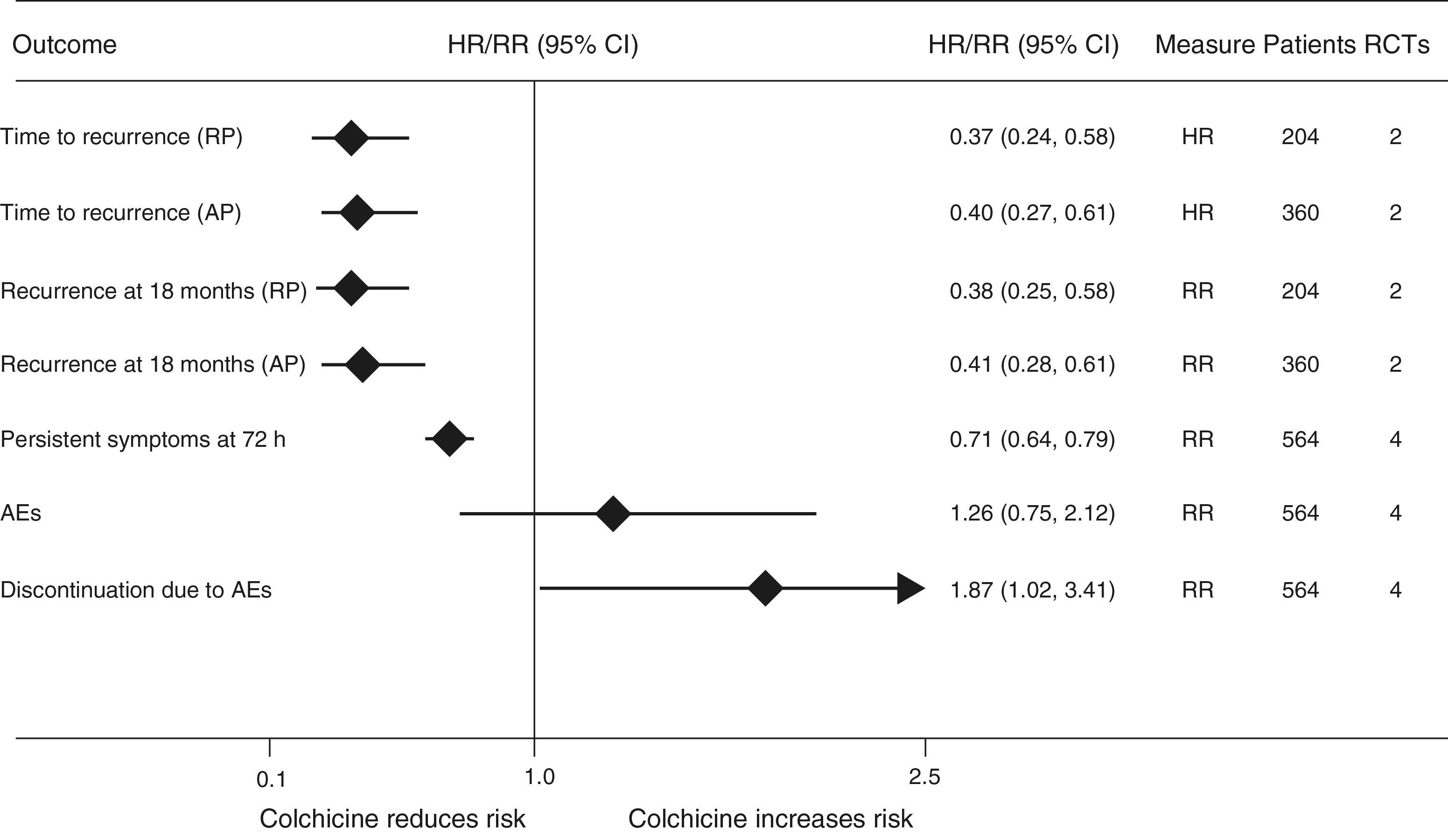
Colchicine significantly reduced time to recurrence in patients with acute pericarditis (HR 0.40; 95% CI (0.27–0.61) and in those with recurrent pericarditis (HR 0.37; 95% CI (0.24–0.58). At 18 months there was a significant reduction in RR of recurrence in patients with acute and recurrent pericarditis (59% and 62%, respectively) (Figure 1). The NNT was 5 for acute [pericarditis] and 4 for recurrent pericarditis.
. AEs: adverse effects; AP: acute pericarditis; CI: confidence interval; HR: hazard ratio; RCTs: randomized controlled trials; RP: recurrent pericarditis; RR: relative risk.")
Effects of colchicine in patients with acute or recurrent pericarditis (adapted from Alabed et al.1). AEs: adverse effects; AP: acute pericarditis; CI: confidence interval; HR: hazard ratio; RCTs: randomized controlled trials; RP: recurrent pericarditis; RR: relative risk.
Colchicine reduced the RR of persistent chest pain by 29% at 72 hours (Figure 1).
With regard to tolerability, total adverse events were not significantly more frequent with colchicine than in controls, but significantly more patients discontinued therapy due to adverse effects (RR 1.87; 95% CI 1.02–3.41).
ConclusionsColchicine as adjunctive therapy to aspirin or NSAIDs at high doses is effective in reducing recurrences in patients with acute or recurrent pericarditis. However, it should be borne in mind that the number of trials on this subject is low and the quality of evidence is sub-optimal.
CommentColchicine is one of the oldest drugs still in the current therapeutic arsenal. It is widely used for the treatment and prevention of acute gout, and its usefulness in other areas is beginning to be explored.
After oral ingestion it has 44% bioavailability, with peak plasma concentration after one hour, and is mainly excreted by the liver. After entering the circulation, colchicine concentrates in leukocytes, where it performs the functions for which it is indicated.2
Colchicine interferes with microtubule dynamics, inhibiting mitosis and neutrophil motility.2 It has additional anti-inflammatory action to that of the standard anti-inflammatories (steroids and NSAIDs), since its mechanism of action does not involve the arachidonic acid pathway.2 The most recent guidelines of the European Society of Cardiology on the diagnosis and management of pericardial diseases (2004) state that colchicine appears to be effective for the treatment of acute pericarditis (class IIa recommendation, level of evidence B) and recurrent pericarditis (class I recommendation, level of evidence B).3
The best available evidence indicates that colchicine significantly reduces the proportion of symptomatic patients after three days of treatment and the long-term recurrence rate, with large reductions in both relative and absolute risk. However, it is associated with a significantly higher rate of discontinuation due to adverse effects, but the fact that total adverse events did not differ from controls, together with the drug's potential clinical benefit, should be weighed against this disadvantage.
The trials under review excluded all patients with pericarditis of bacterial, tuberculous or neoplastic origin, active or severe liver disease, severe renal dysfunction (serum creatinine >2.5 mg/dl), myopathy, bleeding dyscrasia or inflammatory intestinal disease. They also excluded patients with resistant multiple recurrences or with myopericarditis.
Clinical implicationsWhen added to NSAIDs, colchicine reduced persistent symptoms in the short term and the risk of recurrence in the long term in patients with acute pericarditis (maintenance dose for three months) or recurrent (maintenance dose for six months).
Dosages adjusted for body weight (0.5 mg twice daily for patients weighing ≥70 kg and once daily for those weighing <70 kg) appear to have acceptable tolerability. However, due to the potential cumulative risk of iatrogenic gastrointestinal adverse effects with concomitant colchicine and NSAIDs, proton pump inhibitors are recommended in all patients.
Colchicine has not been formally approved for the treatment and/or prevention of events in acute or recurrent pericarditis, and so its use in this context must be considered off-label, despite the existence of moderate quality evidence supporting a favorable risk-benefit ratio.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Caldeira D, Vaz-Carneiro A, Costa J. Cochrane Corner: colchicina na pericardite aguda e recorrente. Rev Port Cardiol. 2015;34:697–699.
