
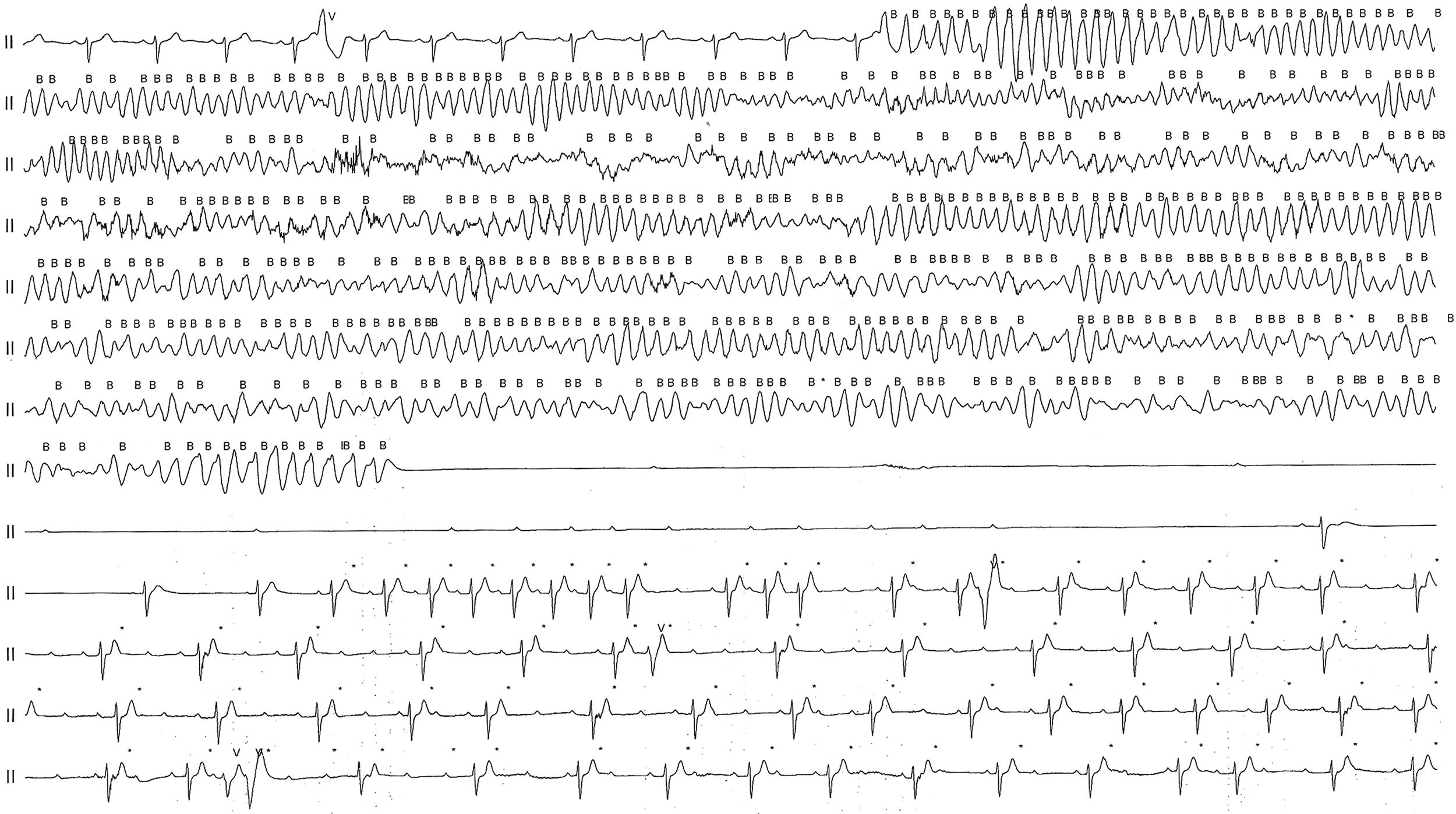
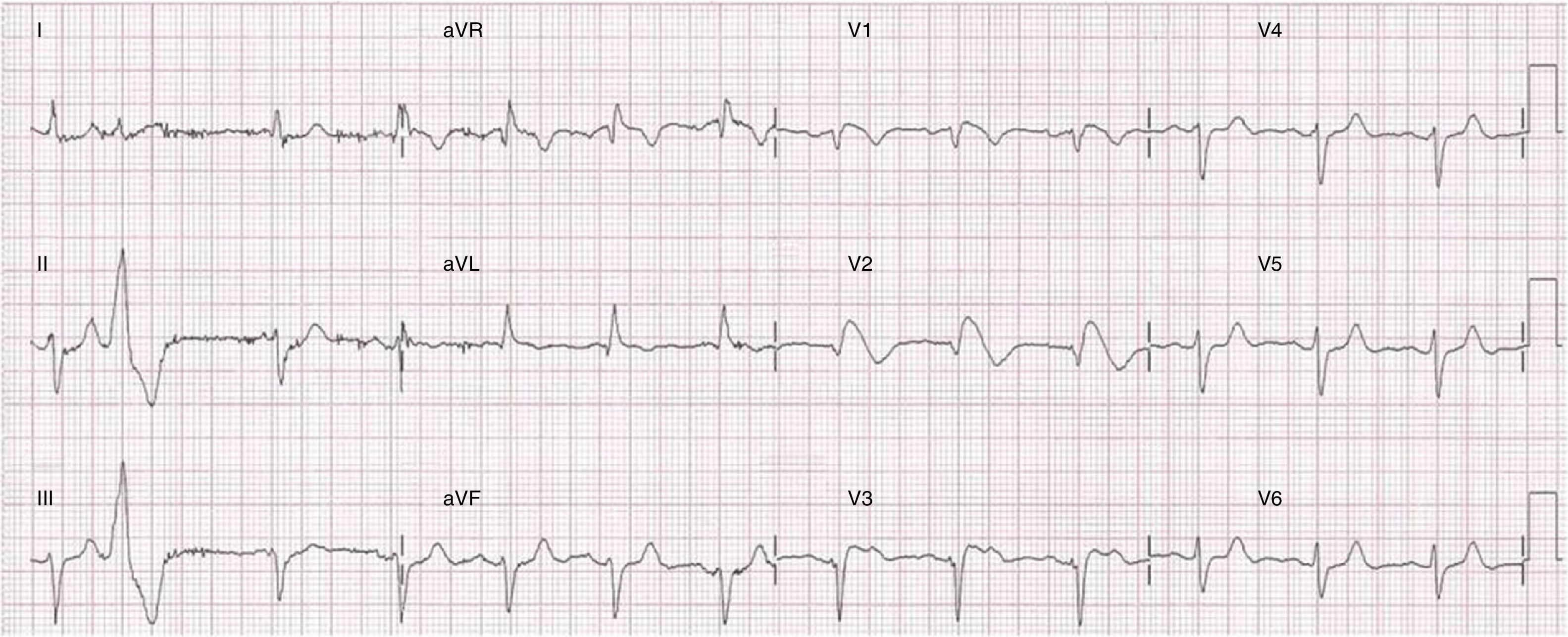
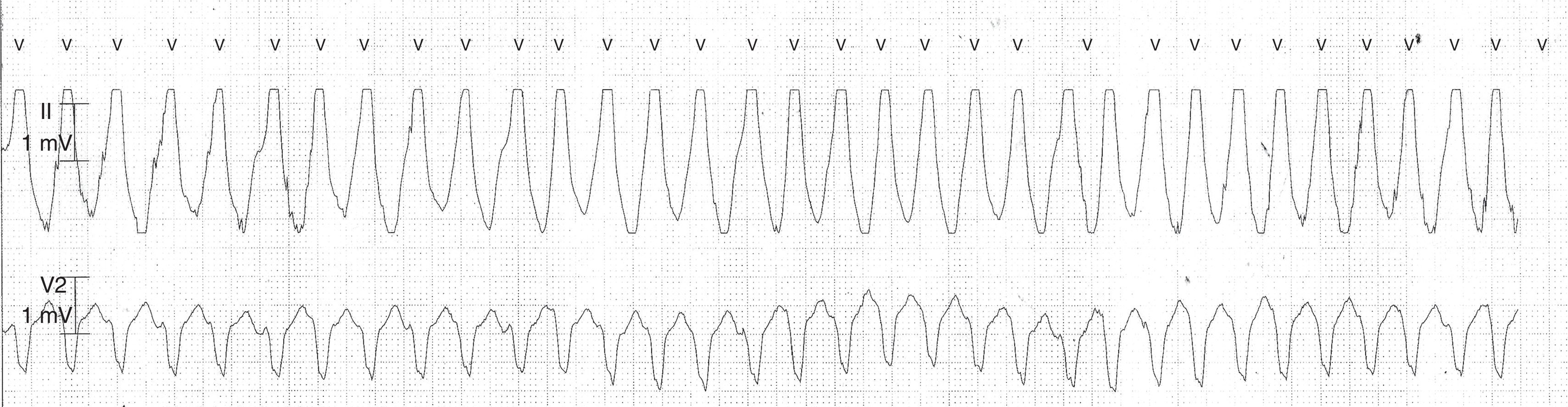
A 60-year-old woman presented with palpitations. Transthoracic echocardiography was normal, a 12-lead electrocardiogram (ECG) was unremarkable and 24-hour Holter monitoring was performed. During monitoring and while asleep, the patient experienced urinary incontinence with no other symptoms. Holter monitoring analysis (Figure 1) revealed a nocturnal episode of polymorphic ventricular tachycardia (VT) followed by ventricular fibrillation (VF) with a duration of two and a half minutes, and asystole (38 seconds). Afterwards, sinus rhythm (SR) resumed with sinoatrial and advanced atrioventricular (AV) block. Ventricular asystole was interrupted by junctional escape beats with AV dissociation, resuming with SR with normal AV conduction. The 12-lead ECG was repeated on the 2nd intercostal space and a type-1 Brugada pattern was documented (Figure 2). There was no evidence of fever or electrolyte imbalance and the use of a QT-prolonging drug was ruled out. Electrical monitoring during hospitalization revealed numerous episodes of monomorphic VT with left bundle branch block morphology and inferior axis (Figure 3). Coronary angiography ruled out significant coronary artery disease and a cardioverter defibrillator was implanted. Electrophysiologic testing was performed with no inducible ventricular arrhythmias. Molecular analysis detected a pathogenic mutation (c.4720G>A) in exon 27 of the SCN5A gene.



Brugada patients have a high risk of sudden cardiac death (SCD) due to polymorphic VT/VF, but its true incidence is difficult to define. This case suggests that patients who appear to be asymptomatic may also experience spontaneously aborted SCD. To our knowledge, this is the first report of spontaneous and complete recovery following a long period of ventricular asystole.
Conflicts of interestThe authors have no conflicts of interest to declare.
