
The obesity and overweight epidemic, together with increasing cardiovascular disease, represent a major public health problem worldwide, and their occurrence in childhood and adolescence has increased in recent decades. The objective of this study was to assess the association between waist-to-height ratio (WHR) and the incidence of hypertension in adolescents.
MethodsWe performed a cross-sectional study of adolescents aged 10-17 years of both sexes attending municipal schools in inland Rio Grande do Sul, Brazil. Using a secondary database, weight and height measurements, blood pressure, and waist circumference (WC) were analyzed and body mass index (BMI) and WHR were calculated. Blood pressure was classified according to the Brazilian hypertension guidelines, BMI according to the curves of the World Health Organization, and WC according to Taylor et al. The cutoff used for WHR was 0.50 for both sexes.
ResultsOf the 1030 adolescents studied, 29.6% (305) presented overweight/obesity and 30.4% (313) had hypertension; 24% (247) had high WC and 18.3% (189) presented high WHR. Participants with WHR ≥0.50 were 2.4 times more likely to have hypertension than those with WHR <0.50 (OR 2.39; 95% CI 1.73-3.32; p<0.001).
ConclusionA positive association was found between WHR and the presence of hypertension in adolescents.
A epidemia de sobrepeso e obesidade, assim como as doenças cardiovasculares, representam um importante problema de saúde pública em todo mundo e a sua prevalência na infância e adolescência vem aumentando nas últimas décadas. O objetivo deste estudo foi avaliar a possível associação entre a razão cintura/estatura (RCE) e a presença de hipertensão (HAS) em adolescentes.
MétodosEstudo transversal envolvendo adolescentes com idade entre 10-17 anos, de ambos os gêneros, pertencentes a escolas municipais do interior do Rio Grande do Sul, Brasil. A partir de banco de dados secundário, foram analisadas as medidas de peso, estatura, pressão arterial e circunferência da cintura (CC), calculou-se o índice de massa corporal (IMC) e a RCE. A classificação da pressão arterial foi feita de acordo com as V Diretrizes Brasileiras de Hipertensão Arterial; o IMC foi classificado de acordo com as curvas da Organização Mundial da Saúde; a CC foi classificada conforme a recomendação de Taylor et al.; e o ponto de corte utilizado para a RCE foi de 0,50 para ambos os gêneros.
ResultadosForam estudados 1030 adolescentes, dentre os quais 29,6% (n=305) apresentavam sobrepeso/obesidade e 30,4% (n=313) hipertensão; 24% (n=247) dos adolescentes apresentaram CC elevada e 18,3% (n=189) apresentaram RCE elevada. Participantes com RCE>0,50 apresentaram uma chance 2,4 vezes maior de HAS, em comparação àqueles com RCE<0,50 (OR=2,39; IC95% 1,73 - 3,32; p<0,001).
ConclusãoAssociação positiva entre RCE e presença de HAS em adolescentes foi observada.
Cardiovascular disease (CVD) is the leading global cause of morbidity and mortality.1 The obesity and overweight epidemic, together with increasing cardiovascular disease, represent a major public health problem worldwide.2,3 Although the clinical manifestations of CVD are generally not seen until adulthood, studies have shown that comorbidities such as dyslipidemia, hypertension and insulin resistance may be present in childhood or adolescence, and that the greater the number of risk factors, the greater the likelihood of developing CVD at a young age.4,5
Obesity is a metabolic disorder characterized by excessive body fat and a chronic inflammatory state.6 There are two types of obesity, central and peripheral. Abdominal obesity is now considered the main risk factor for hypertension in children and adolescents, as confirmed in a cross-sectional study of 1716 adolescents in the city of Cuiabá, Mato Grosso, Brazil.7,8 When adjusted for age, gender and skin color, hypertension was associated with obesity (odds ratio [OR] 2.27; 95% confidence interval [CI] 1.64-3.14) but not with waist circumference (WC) after adjustment for body mass index (BMI).9
Of the indicators used to assess body fat, the waist-to-height ratio (WHR) is a simple and practical tool that uses WC as a measure of abdominal adiposity adjusted to the size of the individual by dividing WC by height.10 WC and WHR are considered important measures to identify overweight adolescents at high cardiometabolic risk.11 Studies have demonstrated that anthropometric indicators can predict hypertension in adolescents.12–15
The objective of this study was to assess the association between WHR and the incidence of hypertension in adolescents.
MethodsWe performed a cross-sectional observational study involving 1030 adolescents aged 10-17 years of both sexes attending municipal schools in inland Rio Grande do Sul, Brazil. The data were extracted from a secondary database established in 2012 and derived from a study which included all students enrolled in municipal schools in September and October 2012 of both sexes and aged between 10 and 17 years. The study was approved by the research ethics committee of Univates, protocol no. 72871 and 151/10, and written informed consent was obtained from parents and guardians. Children not present on the day of data collection, and those who refused or failed to participate in any stage of the study, were excluded.
Blood pressure (BP) was measured using an automatic sphygmomanometer (Omron HEM-742INT) in accordance with the guidelines of the Brazilian Society of Cardiology.3 Subjects were seated in a calm and quiet environment for at least 5 min before assessment, with legs uncrossed and feet flat on the floor, in a chair with their back supported and relaxed, clothing removed from the arm on which the cuff was placed, with the arm supported, hand at the level of the heart and palm upward. They were told not to speak during BP measurement. Those who had physical exercise classes on the day of data collection had their BP measured before or 60-90 min after the exercise session. BP was classified in accordance with the 6th Brazilian Guidelines on Hypertension for each age-group and gender, systolic blood pressure (SBP) and/or diastolic blood pressure (DBP) between the 90th and 95th percentiles being classified as pre-hypertension, between the 95th and 99th percentiles as stage 1 hypertension, and above the 99th percentile as stage 2 hypertension.3
Body weight was assessed using a calibrated digital scale (Urano®), with a maximum capacity of 150 kg and a precision of 100 g. Subjects stood on the center of the scale, without shoes and wearing light clothing. A Sanny® stadiometer was used to measure height, the subjects standing without shoes, heels together, backs straight and arms beside the body.
WC was measured with the subject standing straight, using a flexible non-stretch tape measure with a precision of 1 mm. The bottom of the lowest rib was first located and marked with a pen, then the tape was positioned at the mid-line between the bottom of the lowest rib and the iliac crest and kept horizontal around the abdomen over the navel.
WHR was calculated by dividing WC in cm by height in cm. The cutoff used was 0.50 for both sexes, those with WHR ≥0.50 being classified as at cardiovascular risk and those with WHR <0.50 as not at risk.16
Statistical analysisDescriptive statistics were used to analyze the data (means and standard deviation for quantitative variables and absolute and relative frequencies for qualitative variables). The subjects were compared according to the presence of hypertension using the Student's t test for quantitative variables and the chi-square test for qualitative variables. The correlation between WHR and SBP and DBP was assessed by means of Pearson's correlation coefficient. The strength of the association between WHR and the presence of hypertension was assessed by logistic regression analysis, using the presence of hypertension as the dependent variable and age and gender as covariables. SPSS version 18 was used for the statistical analysis and values of p<0.05 were considered significant.
ResultsOf the 1030 adolescents aged 10-17, mean age 12.43±1.81 years, most (54.7%) were female and most (52%) lived in rural areas.
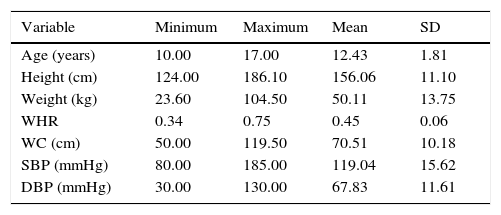
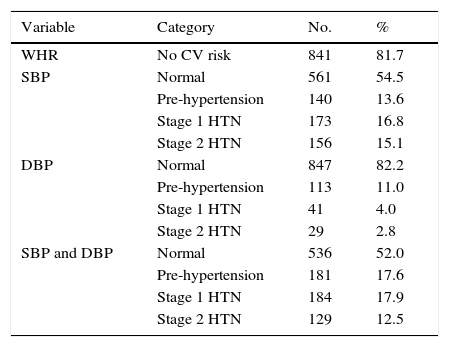
Table 1 presents the anthropometric and BP data of the study population, while Table 2 shows categories of WHR and the presence of hypertension. Most subjects were classified as normal weight (63.8%) and normotensive (52%) based on combined SBP and DBP values. More than 80% of the sample had WHR values indicating no cardiovascular risk and 76% had normal WC values.
Anthropometric and blood pressure data of the study population.
| Variable | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|
| Age (years) | 10.00 | 17.00 | 12.43 | 1.81 |
| Height (cm) | 124.00 | 186.10 | 156.06 | 11.10 |
| Weight (kg) | 23.60 | 104.50 | 50.11 | 13.75 |
| WHR | 0.34 | 0.75 | 0.45 | 0.06 |
| WC (cm) | 50.00 | 119.50 | 70.51 | 10.18 |
| SBP (mmHg) | 80.00 | 185.00 | 119.04 | 15.62 |
| DBP (mmHg) | 30.00 | 130.00 | 67.83 | 11.61 |
DBP: diastolic blood pressure; SD: standard deviation; SBP: systolic blood pressure; WC: waist circumference; WHR: waist-to-height ratio.
Categories of waist-to-height ratio and hypertension in the study population.
| Variable | Category | No. | % |
|---|---|---|---|
| WHR | No CV risk | 841 | 81.7 |
| SBP | Normal | 561 | 54.5 |
| Pre-hypertension | 140 | 13.6 | |
| Stage 1 HTN | 173 | 16.8 | |
| Stage 2 HTN | 156 | 15.1 | |
| DBP | Normal | 847 | 82.2 |
| Pre-hypertension | 113 | 11.0 | |
| Stage 1 HTN | 41 | 4.0 | |
| Stage 2 HTN | 29 | 2.8 | |
| SBP and DBP | Normal | 536 | 52.0 |
| Pre-hypertension | 181 | 17.6 | |
| Stage 1 HTN | 184 | 17.9 | |
| Stage 2 HTN | 129 | 12.5 |
CV: cardiovascular; DBP: diastolic blood pressure; HTN: hypertension; SBP: systolic blood pressure; WHR: waist-to-height ratio.
A weak positive correlation was seen between SBP (r=0.210; p<0.001) and DBP (r=0.136; p<0.001) levels and WHR.
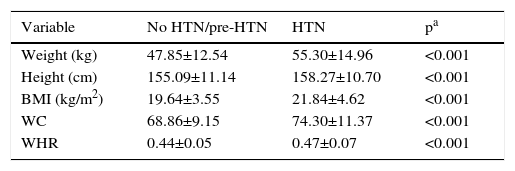
When the study population was grouped according to the presence of hypertension and anthropometric variables were compared, weight, height, BMI, WC and WHR were significantly greater in hypertensive subjects, as shown in Table 3.
Anthropometric variables according to the presence of hypertension.
| Variable | No HTN/pre-HTN | HTN | pa |
|---|---|---|---|
| Weight (kg) | 47.85±12.54 | 55.30±14.96 | <0.001 |
| Height (cm) | 155.09±11.14 | 158.27±10.70 | <0.001 |
| BMI (kg/m2) | 19.64±3.55 | 21.84±4.62 | <0.001 |
| WC | 68.86±9.15 | 74.30±11.37 | <0.001 |
| WHR | 0.44±0.05 | 0.47±0.07 | <0.001 |
BMI: body mass index; HTN: hypertension; WC: waist circumference; WHR: waist-to-height ratio.
The prevalence of childhood obesity has increased in recent decades, and has been called a global epidemic.17 In the present study, 29.6% of adolescents were overweight or obese, a lower figure than in Carneiro et al.18 in a study of 148 adolescents in São Paulo, in which 35.8% were overweight, but higher than in Lima et al.7 in 305 adolescents in Petrolina, Pernambuco (16%) and in Klimek-Piotrowska et al.,19 in 970 Polish adolescents (14.4%). These findings are worrying, since obesity is the main risk factor for hypertension in childhood and adolescence,8 as well as being an independent risk factor for CVD, diabetes, and other disorders.20,21
With regard to abdominal adiposity, 24% of adolescents in the present study had high WC, which puts them at cardiovascular risk. Similar prevalences were found in studies by Bozza et al.21 of 1732 adolescents in Curitiba, Paraná (central obesity in 12.2%) and by Christofaro et al.22 in Londrina, Paraná of 1021 adolescents (15.2% of boys and 8.5% of girls) Table 4.
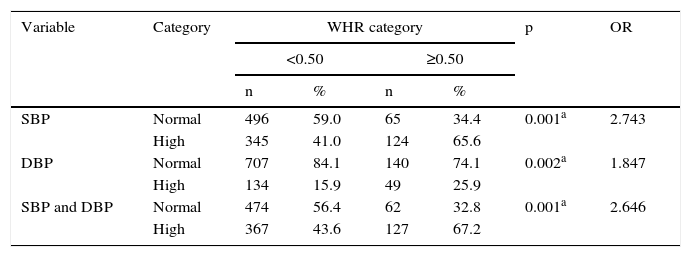
Association between hypertension and high waist-to-height ratio in the study population.
| Variable | Category | WHR category | p | OR | |||
|---|---|---|---|---|---|---|---|
| <0.50 | ≥0.50 | ||||||
| n | % | n | % | ||||
| SBP | Normal | 496 | 59.0 | 65 | 34.4 | 0.001a | 2.743 |
| High | 345 | 41.0 | 124 | 65.6 | |||
| DBP | Normal | 707 | 84.1 | 140 | 74.1 | 0.002a | 1.847 |
| High | 134 | 15.9 | 49 | 25.9 | |||
| SBP and DBP | Normal | 474 | 56.4 | 62 | 32.8 | 0.001a | 2.646 |
| High | 367 | 43.6 | 127 | 67.2 | |||
DBP: diastolic blood pressure; SBP: systolic blood pressure; WHR: waist-to-height ratio.
In the present study, 18.3% of adolescents presented high WHR and thus increased cardiovascular risk, a higher figure than in a study by Mirhosseini et al.23 of 477 adolescent girls in Mashhad, Iran, in which more than 10% had WHR >0.50.
The prevalence of hypertension in the present study was 30.4%, with 17.9% classified as having stage 1 and 12.5% stage 2 hypertension. These figures are higher than those reported by Corrêa Neto et al.15 in a study of 854 adolescents in Rio de Janeiro, of whom 19.4% had hypertension, and by Moura et al.24 in 211 adolescents from north-east Brazil, of whom 13.7% presented hypertension. The prevalence observed in both these studies is high, as the expected prevalence of hypertension in adolescents is around 5%.25 By contrast, Lima et al.7 identified hypertension in only 1% of 305 adolescents in Petrolina, Pernambuco, while Beck et al.12 studied 660 adolescents in Três de Maio, Rio Grande do Sul, and found only 3.3% with hypertension.
Early detection of hypertension is important for control and prevention of hypertension in adulthood, but BP is not routinely measured in most adolescents, which makes the condition difficult to monitor.12
SBP and DBP correlated positively and significantly with WHR in the present study. In a study by Carvalho et al.26 in 968 university students in Maranhão, SBP and DBP were also significantly associated with anthropometric indicators of obesity (BMI, WC, waist-to-hip ratio and WHR). According to Beck et al.,12 WC, BMI and WHR were the best predictors of hypertension in both sexes in 660 adolescents in inland areas of Rio Grande do Sul.
In the present study WHR was significantly associated with BP levels, with more subjects with elevated SBP and DBP and a diagnosis of hypertension among those with WHR ≥0.50 than among those with WHR <0.50. We also showed that participants with WHR ≥0.50 were 2.4 times more likely to have hypertension than those with WHR <0.50 after adjustment for age and gender. In the study by Klimek-Piotrowska et al.19 of 970 Polish adolescents, WHR was the best indicator of obesity in both sexes, while a study by Bacopoulou et al.27 of 1610 adolescents in Greece concluded that WHR was a better predictor of abdominal obesity in both sexes than waist-to-hip ratio.
WHR is a simple, effective and practical screening tool for detecting obesity and metabolic syndrome in children.28 A study by Pelegrini et al.29 of 1197 adolescents in the Brazilian state of Santa Catarina state demonstrated that as well as BMI, WC and WHR can be used to predict high body fat in adolescents, since both are indicators of central obesity.
The present study has the advantage of a large sample size but the potential limitation that only two rather than three BP readings were taken.
In the light of this study's findings and those of similar studies referred to above, it is suggested that adolescents be encouraged to keep their WC to less than half their height.30
ConclusionsA high prevalence of overweight was observed in this sample of adolescents attending municipal schools in inland Rio Grande do Sul, Brazil. Increased cardiovascular risk, as identified by WHR ≥0.50, was positively associated with BP levels, a greater proportion of participants with high WHR having high SBP and DBP and being diagnosed with hypertension. High WHR was associated with a 2.4 times higher likelihood of hypertension than those with normal WHR. We suggest that WHR should be used as an additional tool in the assessment of cardiovascular risk in adolescents, and that they should be encouraged to keep their WC to less than half their height.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Gomes Madruga J, Moraes Silva F, Scherer Adami F. Associação positiva entre razão cintura-estatura e presença de hipertensão em adolescentes. Rev Port Cardiol. 2016;35:479–484.
