
Levosimendan is a pyridazinone-dinitrile derivative with positive inotropic and vasodilatory effects that has beneficial effects on myocardial performance.
In previous randomized studies levosimendan improved hemodynamics and clinical course, but its effect on prognosis is still unclear. This important issue has limited its use. Although primarily used in the management of acute heart failure syndromes, this new inotropic agent may play a role in other clinical conditions.
This review aims to summarize current knowledge on levosimendan and to present future prospects for the use of this drug.
O levosimendan é um derivado da piridazinona-dinitrilo que induz um efeito inotrópico positivo e vasodilatador, exercendo efeitos benéficos sobre o desempenho do miocárdio.
Em estudos aleatorizados prévios o levosimendan melhorou a hemodinâmica e a evolução clínica dos doentes, com um significado ainda pouco definido no prognóstico. Esta questão importante tem condicionado o seu uso. Embora seja utilizado principalmente no tratamento da insuficiência cardíaca aguda, este novo agente poderá desempenhar um papel importante em outras condições clínicas.
Esta revisão pretende resumir o conhecimento atual sobre o levosimendan e mostrar perspetivas futuras no uso deste fármaco.
Levosimendan is a novel inotrope that is effective in the treatment of acute heart failure (HF), with clear hemodynamic and clinical benefits. In spite of this, a lack of concrete data on prognosis has limited its application in clinical practice, and the most recent European Society of Cardiology (ESC) guidelines for the treatment of HF in fact downgraded the class of recommendation and level of evidence for its use.1
Despite this, levosimendan is a drug with unique pharmacodynamic and pharmacokinetic characteristics that definitely warrants further trials and validation. This review aims to summarize current knowledge on the therapeutic actions of levosimendan in HF, as well as to explore potential off-label uses and future prospects.
Mechanism of action and pharmacokineticsLevosimendan is a pyridazinone-dinitrile derivative class III Ca2+ sensitizer that increases the affinity of troponin C (TnC) for Ca2+. It binds to the N-terminal domain of cardiac TnC in a Ca2+ concentration-dependent manner, stabilizing the TnC-Ca2+ complex and inhibiting troponin I.2,3 It thereby accelerates the actin-myosin crossbridge formation rate and decelerates the dissociation rate. This positive inotropic effect is not due to Ca2+ overload, nor does it occur at the expense of an increase in myocardial O2 demand.4–7 Its actions depend on intracellular Ca2+ levels and as Ca2+ levels decrease during diastole, levosimendan does not impair ventricular relaxation.3,8 In fact, it has been shown that levosimendan improves diastolic function.9
Beyond increasing the affinity of TnC for Ca2+, levosimendan activates ATP-sensitive K+ channels in the vascular smooth muscle sarcolemma, leading to cell hyperpolarization and vasodilation and reducing peripheral vascular resistance. Levosimendan relaxes both arterial and venous smooth muscle cells, leading to a decrease in both preload and afterload10,11 and increasing stroke volume and cardiac output (CO).12 It may protect the myocardium from ischemia as it dilates the coronary arteries and improves O2 supply.13 It also opens myocardial mitochondrial ATP-sensitive K+ channels, thereby protecting cardiomyocytes against apoptosis, ischemia-reperfusion injury and oxidative stress.14
Additionally, although levosimendan selectively inhibits phosphodiesterase type 3, thus increasing intracellular cyclic adenosine monophosphate (cAMP) and Ca2+, these effects are minor at usual doses.15
Although levosimendan's elimination half-life is only about one hour, its hemodynamic effects last for days. About 5% of the drug is metabolized in the intestine into OR-1855 and subsequently acetylated in the liver to form OR-1896.16 This second metabolite has a half-life of approximately 80 hours and shares most of levosimendan's hemodynamic actions,17 allowing for long-lasting effects after a 24-hour infusion. Acetylation of OR-1855 into OR-1896 shows individual variation; while most Caucasians are slow acetylators, Asians are typically fast acetylators.18 The hemodynamic effects, however, are similar in both groups.19 Also, hepatic dysfunction does not warrant a dose adjustment even if the elimination half-life of metabolites is prolonged.20 Importantly, while some inotropes exhibit tolerance after an infusion of several hours, this was not shown for levosimendan. Lastly, withdrawal is not followed by a rebound effect.14
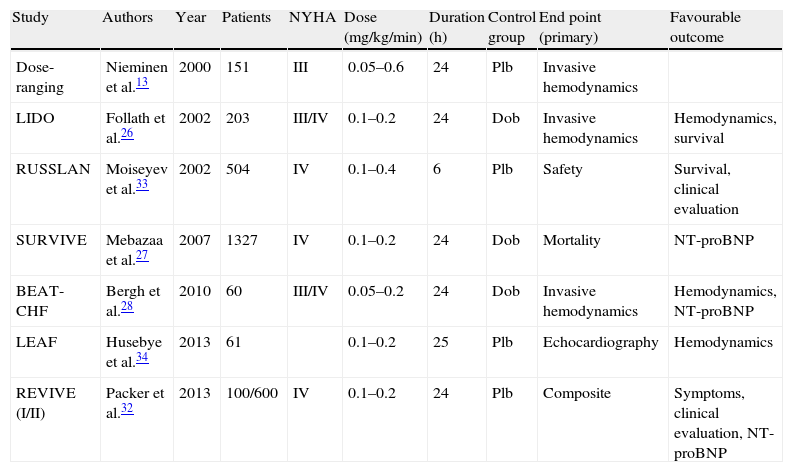
Clinical evidenceLevosimendan has been very successful in the management of acute HF syndromes, leading to sustained improvement in hemodynamics and symptoms and reduced levels of B-type natriuretic peptide (BNP) and other neurohumoral markers of HF compared with standard inotropes (Table 1).21–24 Nevertheless, its long-term effects on cardiac remodeling and cardiovascular mortality remain largely unknown.
Summary of randomized controlled clinical trials with levosimendan.
| Study | Authors | Year | Patients | NYHA | Dose (mg/kg/min) | Duration (h) | Control group | End point (primary) | Favourable outcome |
| Dose-ranging | Nieminen et al.13 | 2000 | 151 | III | 0.05–0.6 | 24 | Plb | Invasive hemodynamics | |
| LIDO | Follath et al.26 | 2002 | 203 | III/IV | 0.1–0.2 | 24 | Dob | Invasive hemodynamics | Hemodynamics, survival |
| RUSSLAN | Moiseyev et al.33 | 2002 | 504 | IV | 0.1–0.4 | 6 | Plb | Safety | Survival, clinical evaluation |
| SURVIVE | Mebazaa et al.27 | 2007 | 1327 | IV | 0.1–0.2 | 24 | Dob | Mortality | NT-proBNP |
| BEAT-CHF | Bergh et al.28 | 2010 | 60 | III/IV | 0.05–0.2 | 24 | Dob | Invasive hemodynamics | Hemodynamics, NT-proBNP |
| LEAF | Husebye et al.34 | 2013 | 61 | 0.1–0.2 | 25 | Plb | Echocardiography | Hemodynamics | |
| REVIVE (I/II) | Packer et al.32 | 2013 | 100/600 | IV | 0.1–0.2 | 24 | Plb | Composite | Symptoms, clinical evaluation, NT-proBNP |
LIDO, Levosimendan Infusion versus DObutamine; RUSSLAN, Randomised stUdy on Safety and effectivenesS of Levosimendan in patients with left ventricular failure due to an Acute myocardial iNfarct; SURVIVE, Survival of patients with acute heart failure in need of intravenous inotropic support; BEAT-CHF, Better Effectiveness After Transition – Heart Failure; LEAF, LEvosimendan in Acute heart Failure following myocardial infarction; REVIVE I and II, Randomized EValuation of Intravenous LeVosimendan Efficacy I and II; Plb, placebo; Dob, dobutamine; NT-proBNP, N-terminal pro-type B natriuretic peptide.
The effect of levosimendan compared with beta-adrenergic agonists is still the subject of debate. In the Levosimendan Infusion versus DObutamine (LIDO) trial, levosimendan led to greater improvement in hemodynamics and in secondary and post-hoc analyses it was associated with a lower risk of death at 31 and 180 days,25 whereas in the SURVIVE trial no difference between levosimendan and dobutamine groups was found for survival during long-term follow-up despite evidence for an early reduction in plasma BNP levels with levosimendan.26 However, in both studies, the subgroup of patients receiving concomitant beta-blockers showed lower mortality when treated with levosimendan compared to dobutamine. This was not shown in the BEAT-CHF trial, in which there was no superiority of levosimendan over dobutamine, with only a trend in favor of levosimendan at 24 hours after the start of drug infusion. However, this study had a major bias in patient recruitment.27 A recent meta-analysis demonstrated a long-term survival benefit of levosimendan over dobutamine and placebo in patients requiring inotropic support.28 This study also showed that levosimendan treatment is associated with a reduced hospital length of stay (LOS). Another meta-analysis suggested that in critically ill patients requiring inotropic support, levosimendan improves survival compared to dobutamine.29 This benefit was also shown in subgroups of patients such as those with ischemic HF, post-cardiac surgery and those under concomitant beta-blockade.29 Therefore, levosimendan may be considered as an alternative to dobutamine in acutely decompensated HF patients chronically receiving beta-blockers.30 According to the 2012 ESC guidelines on HF, levosimendan is considered in acute HF without severe hypotension when beta-blockade is thought to contribute to hypoperfusion (class IIb, level of evidence C).1
The results from other studies vary. A secondary analysis of the REVIVE trial showed that levosimendan improves symptoms in acutely decompensated HF, at the expense of an increase in adverse side-effects such as hypotension, tachycardia and arrhythmia.31 In the RUSSLAN trial levosimendan was well tolerated and effective in HF after acute myocardial infarction (MI). It was the first inotrope to decrease mortality after MI compared with placebo.32 The LEAF trial also showed that levosimendan is well tolerated and improves regional contractility in post-ischemic myocardium after percutaneous coronary intervention in ST-segment elevation MI complicated by HF.33
A concern regarding levosimendan is cost-effectiveness. A cost-effectiveness analysis of the REVIVE II trial on the use of levosimendan showed shorter hospital LOS and lower cost for the initial hospital admission compared to standard of care.34
Side-effectsUnlike standard inotropes such as dobutamine or milrinone, levosimendan does not increase myocardial O2 consumption and is less pro-arrhythmic.5–7,35,36 Although some studies show increased ventricular tachycardia with levosimendan compared with placebo,31 others do not.26,33 This discrepancy may be due to different infusion rates. In the PORTLAND trial a 0.1 μg/kg/min infusion rate proved to be clinically effective and safe with no pro-arrhythmic effects.37
Two major concerns with the use of levosimendan are hypokalemia and hypotension. The mechanism underlying hypokalemia is still unknown. Hypotension due to vasodilation and increased diuresis is more pronounced when a bolus is administered, and the new ESC guidelines on acute and chronic HF do not recommend bolus administration.1
Renal blood flow and glomerular filtration rate are improved both acutely38 and chronically39 by levosimendan more than by dobutamine.40 Levosimendan is reno-protective through activation of ATP-sensitive K+ and potent vasodilation, which leads to increased renal perfusion, and possibly through its anti-inflammatory effects.40,41
New prospectsOral and other forms of administrationAs chronic therapy for advanced HF, it has been demonstrated that intermittent levosimendan infusions are safe and improve ventricular function and quality of life.42,43
Levosimendan is most commonly administered intravenously, but its use via inhalation has also been shown to improve survival and to attenuate inflammation, particularly in acute lung injury.44
Additionally, levosimendan can also be given orally, which is useful for chronic therapy. Chronic oral levosimendan has shown promising results in both animal and human studies,45–47 preventing post-infarction HF, cardiomyocyte hypertrophy and apoptosis in spontaneously type 2 diabetic Goto-Kakizaki rats45 and improved survival by preventing cardiac remodeling and cardiomyocyte apoptosis in hypertensive Dahl/Rapp rats.46 In the PERSIST trial levosimendan decreased BNP levels and improved quality of life in patients with severe chronic HF, although no symptomatic improvement was shown compared to placebo.47 Oral levosimendan was also shown to reduce filling pressures as assessed by echocardiographic indices and systolic function in chronic HF patients.48
Despite expectations it has been difficult to establish an optimal oral dosing regimen, and further research on safety and efficacy in HF patients is warranted. The ongoing LION-HEART (ClinicalTrials.gov Identifier: NCT01536132) and LevoRep (ClinicalTrials.gov Identifier: NCT01065194) trials aim to determine the safety and efficacy of intravenous administration of intermittent doses of levosimendan compared to placebo in ambulatory patients with severe chronic HF.
Effects of levosimendan in cardiac surgeryPatients undergoing cardiac surgery frequently require inotropic support immediately after cardiopulmonary bypass. The commonly used inotropes enhance myocardial contractility by increasing cAMP concentration, which increases myocardial O2 consumption and further disrupts the supply-demand balance, especially in the failing myocardium.49 Levosimendan may have an advantage due to its distinct mechanism of action, enhancing myocardial performance, and offers a promising therapeutic option during off-pump coronary artery bypass grafting (CABG) in patients with normal or impaired myocardial function.50,51
Although the results are still controversial, most studies on levosimendan in cardiac surgery show a cardioprotective effect, with a decrease in the incidence of low CO syndromes and reduced cardiac troponin release in the postoperative setting that may reduce postoperative mortality.52–54
It has also been shown that pretreatment with levosimendan in patients undergoing CABG reduces myocardial injury, tracheal intubation time, requirement for inotropic support, and hospital LOS in the intensive care unit.55
Right ventricular dysfunction and pulmonary hypertensionRight ventricular (RV) dysfunction is an indicator of poor prognosis in advanced HF. Several studies have shown that levosimendan improves echocardiographic and hemodynamic markers of RV function when administered to patients with advanced HF and compromised RV function, since it dilates pulmonary vessels and improves biventricular function.56,57 In experimental models of acute RV dysfunction due to RV MI in pigs, levosimendan improved global hemodynamics and optimized RV ventriculo-vascular coupling (VVC) by the double effect of increased contractility and reduced RV afterload.58,59 Further, in an experimental setting of acute pulmonary embolism and pulmonary hypertension (PH), levosimendan restored RV VVC due to the combination of pulmonary artery vasodilation and increased RV contractility.60
In case reports levosimendan shows a clear benefit during mitral valve surgery in patients with severe PH by reducing pulmonary artery pressure (PAP) and protecting RV contractility.61,62 However, in another case report of patients with idiopathic pulmonary arterial hypertension, levosimendan failed to reduce PAP.63
Levosimendan has been shown to be superior to dobutamine in some patient groups: in children with PH undergoing cardiac surgery64 and in patients with biventricular failure levosimendan improves ejection fraction and tricuspid annular plane systolic excursion, decreasing systolic PAP.65
Nevertheless, the role that levosimendan may play in PH with preserved left ventricular function has been little investigated, particularly in chronic PH. It has been reported that levosimendan attenuates pulmonary vascular remodeling due to antiproliferative and anti-inflammatory effects in a rat model of monocrotaline-induced PH.66 Furthermore, in a pilot study enrolling patients with HF due to PH of various etiologies, repeated administration of levosimendan was effective in improving hemodynamics.67 Its role in patients with chronic PH of other etiologies, particularly idiopathic, is unknown, but its positive inotropic effects and vasodilation of the pulmonary arteries suggest beneficial effects.68
ConclusionsAlthough further studies are needed, current clinical evidence suggests that levosimendan is more effective than classical inotropes in improving cardiac mechanical efficiency and reducing congestion in acute HF patients without hypotension. Emerging new off-label uses in conditions such as PH and cardiac surgery may soon expand its clinical applicability. Further studies should be carried out in these patient groups.
Conflicts of interestThe authors have no conflicts of interest to declare.
This work was supported by the Portuguese Foundation for Science and Technology (Grants PEst-OE/SAU/UI0051/2014 and EXCL/BIM-MEC/0055/2012, partially funded by FEDER through COMPETE) through the Cardiovascular R&D Unit and by the European Commission (Grant FP7-Health-2010; MEDIA-261409).
