
We describe the case of a 76-year-old woman, diagnosed with a neuroendocrine tumor of the cecum in 2004, with liver metastases and carcinoid syndrome since September 2010. The patient had been treated intermittently with chemotherapy cycles, and remained symptomatic, with worsening secondary lesions. In June 2011 she began to present signs and symptoms of right heart failure and was hospitalized in September 2011. Transthoracic two- and three-dimensional echocardiography revealed enlarged right atrium and ventricle and thickened and fixed tricuspid and pulmonary valve leaflets, causing severe tricuspid regurgitation and mild pulmonary regurgitation and stenosis, suggestive of carcinoid heart disease. The authors discuss the clinical importance of transthoracic echocardiography, and the more recent three-dimensional echocardiography as the diagnostic exam of choice in these cases, as it is especially suitable for assessing the valves and subvalvular apparatus.
Os autores apresentam o caso de uma doente de 76 anos, com o diagnóstico de tumor neuroendócrino do cego desde 2004 com metastização hepática, e com síndrome carcinóide desde setembro de 2010. A doente realizou ciclos de quimioterapia de forma intermitente, pelo que manteve sintomas e agravamento das lesões secundárias. Desde junho de 2011 apresenta sinais e sintomas compatíveis com insuficiência cardíaca direita, ficando internada em setembro de 2011. Nesta sequência realizou ecocardiograma transtorácico bi e tridimensional que revelou cavidades direitas dilatadas e folhetos das válvulas tricúspide e pulmonar espessados, fixos, condicionando insuficiência tricúspide grave e estenose e insuficiência pulmonar ligeiras, sugestivas de doença carcinóide cardíaca. Os autores discutem a relevância clínica da ecocardiografia transtorácica, e, atualmente, da ecocardiografia tridimensional, como o método de investigação de escolha nestes casos, ao permitir avaliar de forma única as válvulas e o aparelho subvalvular.
Carcinoid tumors, with an incidence in the general population of 1/100000 individuals, are rare malignant neoplasms that arise from enterochromaffin cells located in the gastrointestinal tract or lungs.1,2
At the time of diagnosis, 20–30% of patients have disseminated disease and present with carcinoid syndrome, characterized by flushing, diarrhea and bronchospasm. This syndrome is caused by tumor release of serotonin and other vasoactive substances.3
Approximately 50–60% of patients with the syndrome present carcinoid heart disease, which is caused by vasoactive substances secreted by metastatic tumor cells in the liver reaching the right heart, leading to deposition of fibrous tissue in the endocardium. Studies suggest that the prevalence of carcinoid heart disease is decreasing following the introduction of somatostatin analogs and other antitumor therapies designed to reduce the tumor load and the production of tumor secretory products.4,5
Carcinoid heart disease is initially well tolerated, and patients may remain in New York Heart Association (NYHA) functional class I, even with severe valvular lesions in the right heart. However, typical signs and symptoms of right heart failure appear as the disease progresses.
The echocardiographic features are well defined: classically the tricuspid and pulmonary subvalvular apparatus and valve leaflets are thickened and fixed, limiting leaflet excursion and preventing coaptation, which can cause a combination of valve regurgitation and stenosis. In most patients with carcinoid heart disease, the tricuspid valve is affected, with or without pulmonary valve involvement. Around 15% of patients have valve lesions in the left heart, also characterized by diffuse leaflet thickening, although less severe than in the right heart. Mild pericardial effusion occurs in 10% of patients, but cardiac metastases are rare.4
We present the case of a female patient with carcinoid syndrome in whom transthoracic two- and three-dimensional echocardiography provided sufficiently accurate assessment of valve structures to establish a diagnosis of carcinoid heart disease without the need for transesophageal echocardiography.
Case reportWe describe the case of a 76-year-old woman, with no relevant personal history, diagnosed with a neuroendocrine tumor of the cecum with an insular pattern in January 2004 following right hemicolectomy, and followed since then in medical oncology consultations.
Abdominal computed tomography and 111In-pentetreotide scintigraphy (octreoscan) revealed metastasization to the liver, and palliative treatment was begun with five million units (MU) interferon-alfa three times a week. In April 2004 the patient underwent excision of five liver metastases, bilateral oophorectomy and excision of a peritoneal nodule. Histological study of all fragments revealed carcinoid tumor, and so interferon-alfa therapy was maintained.
In March 2005, on repeat octreoscan no liver lesions were observed, and the patient continued to be monitored. In January 2007, although clinically asymptomatic, she presented liver uptake on octreoscan and elevated 5-hydroxy-indolacetic acid, an indication for interferon or chemotherapy, but the patient refused any treatment.
In September 2010, she presented sporadic episodes of flushing, diarrhea and bronchospasm and octreotide therapy was begun for carcinoid syndrome, but despite slight symptomatic improvement, the therapy was discontinued in December 2010 due to intolerance (nausea, vomiting and abdominal pain).
In January 2011, the patient complained of fatigue on progressively less exertion and showed disease progression with worsening liver lesions; oral chemotherapy was begun with capecitabine, but was discontinued after four cycles due to intolerance (nausea, vomiting and diarrhea). She still had symptoms of carcinoid syndrome and worsening secondary lesions, but refused directed therapy.
In June 2011, the patient began to present lower limb edema, increased abdominal volume and worsening fatigue, and was admitted in September 2011 with a provisional diagnosis of decompensated heart failure.
Physical examination showed pale and dry mucous membranes, liver palpable 4cm below the right costal margin, positive fluid wave sign and lower limb edema up to the hip joint.
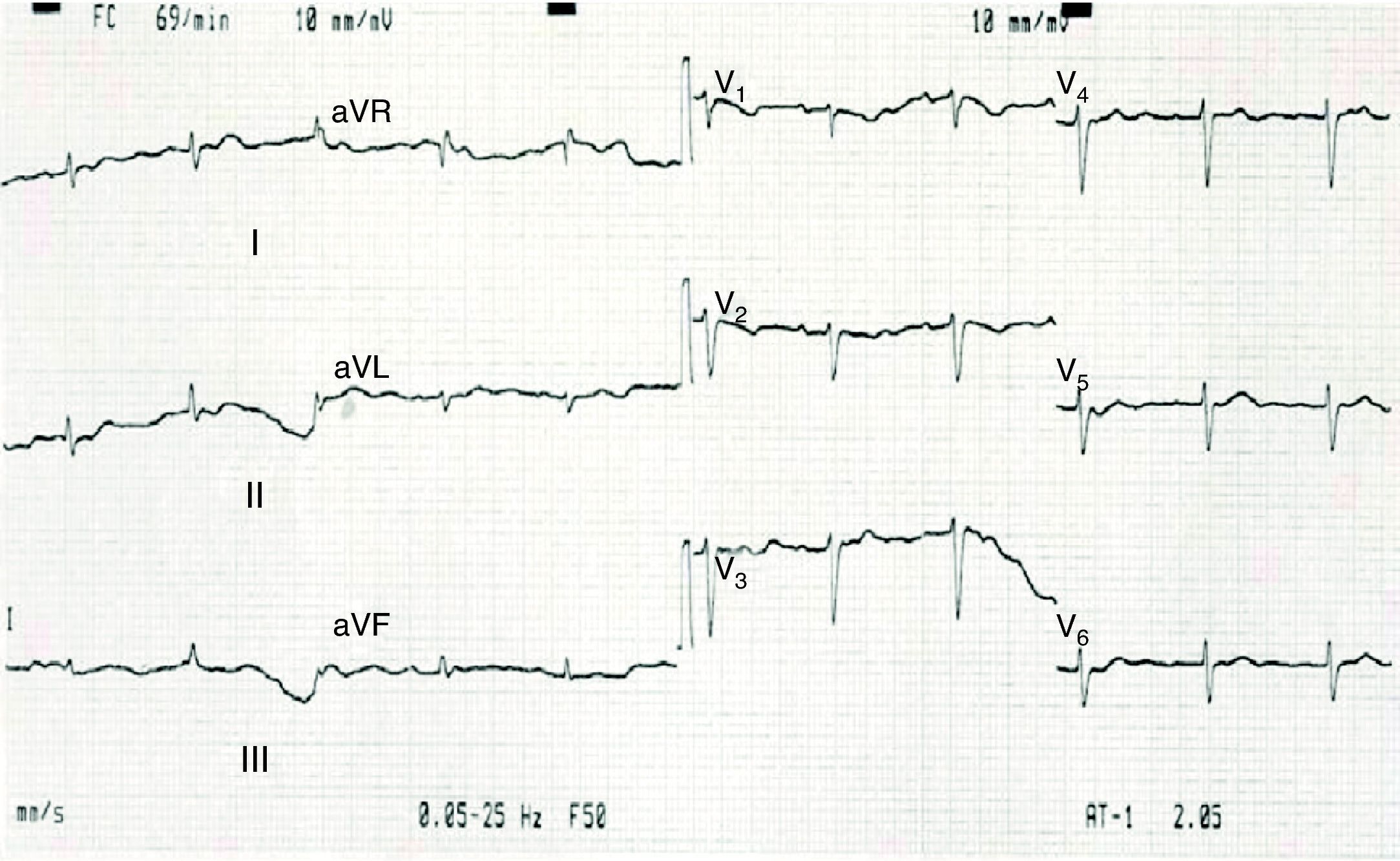
Diagnostic exams included an electrocardiogram on admission (Figure 1), which showed sinus rhythm, heart rate of 70bpm, and low QRS voltage in all leads.

The admission chest X-ray revealed obliteration of both costophrenic angles, compatible with bilateral pleural effusion.
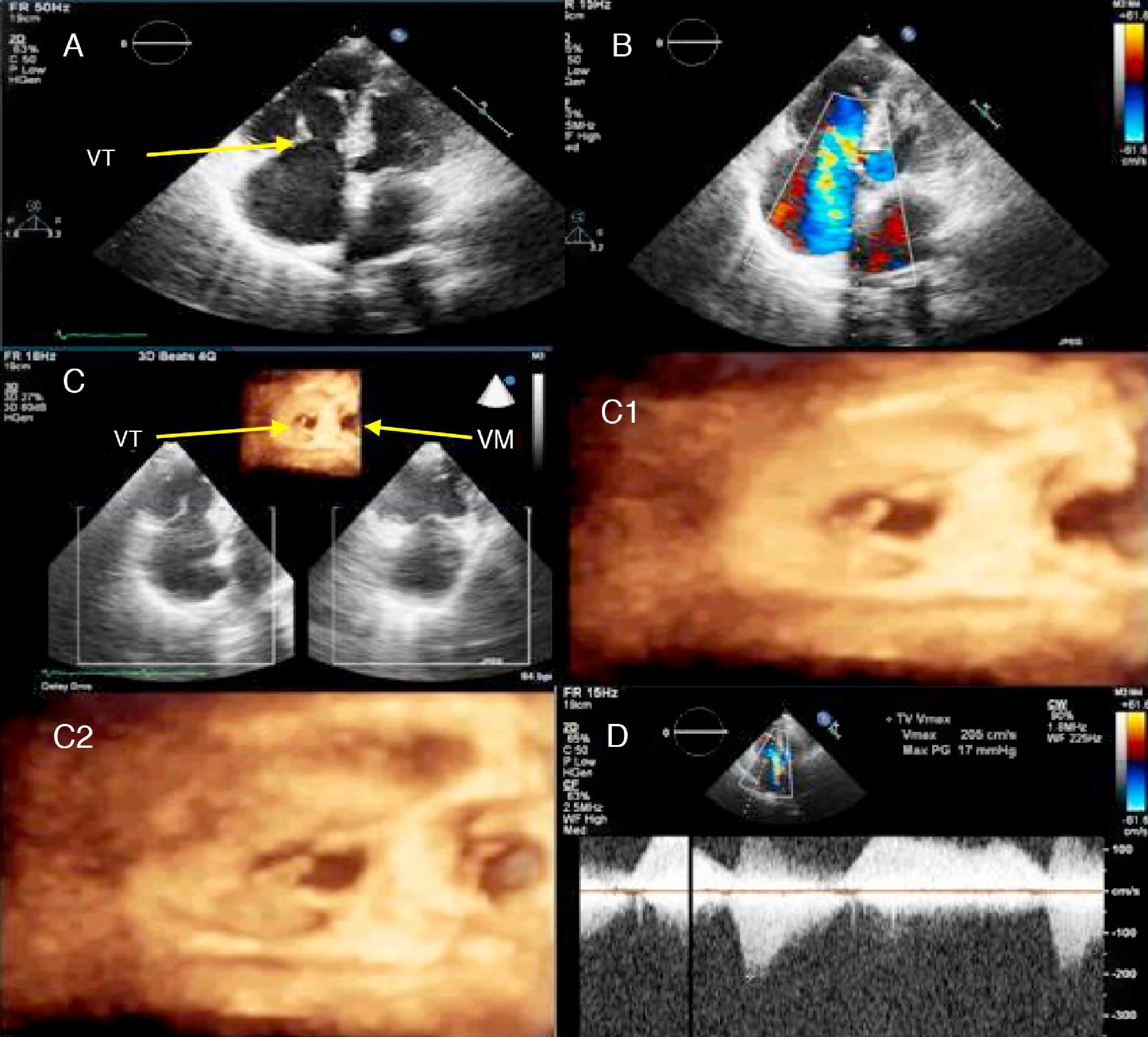
Transthoracic two- and three-dimensional echocardiography (Figures 2 and 3) showed normal left ventricular dimensions and wall thickness, with no wall motion abnormalities and preserved global systolic function. The right chambers were enlarged (Figure 2A), with good right ventricular global systolic function (tricuspid annular plane systolic excursion: 22mm), with no significant gradient between the right ventricle and right atrium (Figure 2D). The tricuspid valve leaflets were visibly thickened, preventing coaptation in systole and causing severe tricuspid regurgitation (Figure 2B), which was more evident in three-dimensional images (Figure 2C1 and C2).
 apical 4-chamber view in systole, revealing right chamber dilatation, thickened tricuspid valve leaflets preventing coaptation, fixed in semi-open position; (B) color Doppler echocardiography, showing severe tricuspid regurgitation; (C) three-dimensional echocardiography, comparing the tricuspid and mitral valves, viewed from the ventricular side: (C1) detail in diastole, showing fixed tricuspid valve leaflets, thickened in comparison to mitral valve leaflets; (C2) detail in systole, revealing mitral valve closure and non-closure of the tricuspid valve; (D) color Doppler echocardiography, showing tricuspid regurgitation. VM: mitral valve; VT: tricuspid valve.")
Carcinoid involvement of the tricuspid valve: (A) apical 4-chamber view in systole, revealing right chamber dilatation, thickened tricuspid valve leaflets preventing coaptation, fixed in semi-open position; (B) color Doppler echocardiography, showing severe tricuspid regurgitation; (C) three-dimensional echocardiography, comparing the tricuspid and mitral valves, viewed from the ventricular side: (C1) detail in diastole, showing fixed tricuspid valve leaflets, thickened in comparison to mitral valve leaflets; (C2) detail in systole, revealing mitral valve closure and non-closure of the tricuspid valve; (D) color Doppler echocardiography, showing tricuspid regurgitation. VM: mitral valve; VT: tricuspid valve.
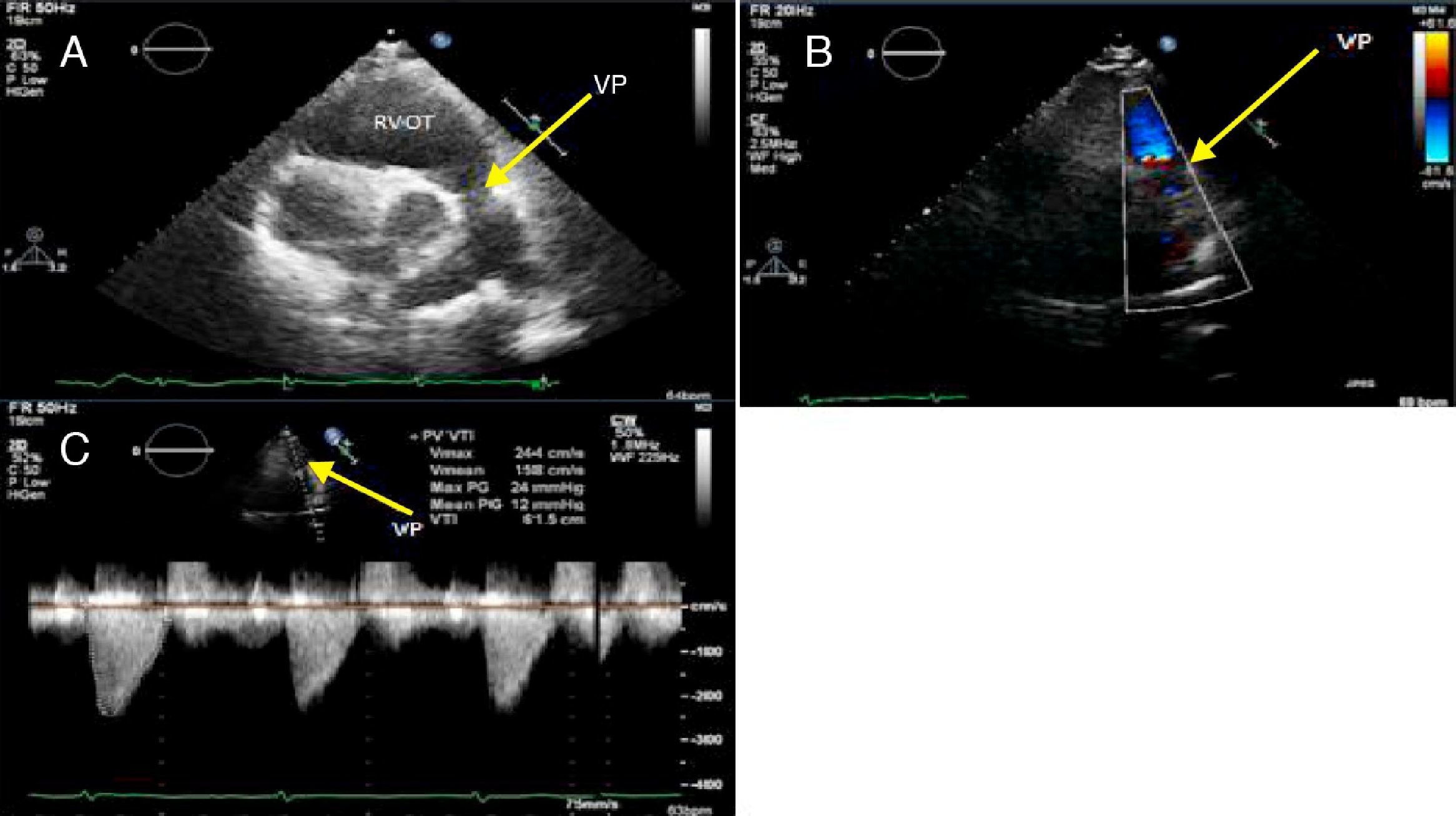
 right ventricular outflow tract, showing thickened pulmonary valve leaflets; (B) color Doppler echocardiography, showing mild pulmonary regurgitation with slightly turbulent diastolic flow; (C) continuous wave Doppler echocardiography, revealing mild pulmonary stenosis. RVOT: right ventricular outflow tract; VP: pulmonary valve.")
Carcinoid involvement of the pulmonary valve: (A) right ventricular outflow tract, showing thickened pulmonary valve leaflets; (B) color Doppler echocardiography, showing mild pulmonary regurgitation with slightly turbulent diastolic flow; (C) continuous wave Doppler echocardiography, revealing mild pulmonary stenosis. RVOT: right ventricular outflow tract; VP: pulmonary valve.
The pulmonary valve cusps were thickened, causing mild pulmonary stenosis (Figure 3C) and regurgitation (Figure 3B).
The patient was medicated with furosemide (40mg/day), ramipril (10mg/day) and spironolactone (50mg/day), but still refused any other treatment. She was discharged, clinically improved, on October 28, 2011.
Discussion and ConclusionsBesides the structural lesions of carcinoid heart disease (thickening of the endocardium, with deposition of fibrous tissue, classically involving the right heart), other cardiovascular effects include major hemodynamic changes.6,7
Without intervention or directed therapy, the disease progresses and can lead to symptomatic right heart failure,4 as in the case presented here, of a female patient who presented low QRS voltage on the admission electrocardiogram, a change that is very common in patients with carcinoid heart disease and one of the initial clues for its diagnosis, despite its low sensitivity.
The valve abnormalities most often found in the disease were also present: tricuspid regurgitation (the tricuspid valve is involved in almost all cases) and pulmonary stenosis.
In many cases, as in this one, thickening of the leaflets and subvalvular apparatus leads to retraction of the leaflets, which become fixed, preventing coaptation and leaving the valve in a semi-open position. In functional terms, there may be a combination of valve regurgitation and stenosis, resulting in significant hemodynamic compromise. Pulmonary stenosis is thought to worsen tricuspid regurgitation, and the severity of pulmonary stenosis may be underestimated due to low cardiac output and severe tricuspid regurgitation.
The right atrium and ventricle are typically enlarged, with paradoxical motion of the interventricular septum due to right ventricular volume overload. Nevertheless, right ventricular function is preserved until the late stages of the disease.4
Although the diagnosis is frequently made by transthoracic echocardiography, cardiac computed tomography and magnetic resonance imaging can provide important additional anatomical and functional information, particularly for assessment of valve structures, right ventricular function and right chamber volumes.4,8
Chromogranin-A (CgA) has been established as a marker for diagnosis of neuroendocrine tumors for several years, while N-terminal pro-brain natriuretic peptide (NT-proBNP) is an excellent biomarker of ventricular dysfunction. Korse et al. assessed the diagnostic and prognostic value of CgA and NT-proBNP in patients with carcinoid heart disease and tricuspid regurgitation, concluding that both are important for diagnosis and that elevated levels of both markers are associated with worse prognosis.9
The case presented highlights the importance of transthoracic echocardiography, and particularly three-dimensional echocardiography, for the diagnosis of carcinoid heart disease and accurate assessment of valve lesions.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Santos, A.R. Coração carcinóide – a propósito de um caso clínico. Rev Port Cardiol 2012. http://dx.doi.org/10.1016/j.repc.2012.01.020.
